Three Dimensional Contrast Angiography
Mark Doyle
OVERVIEW
Contrast angiography relies on administering a contrast agent that is imaged in a three-dimensional (3D) manner. Here we discuss the acquisition and contrast mechanism, and examine the issues associated with timing the sequence to maximize contrast. Lastly, approaches to rendering the 3D data sets will be discussed.
BASIC PRINCIPLES
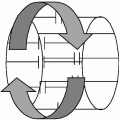
The conventional 2D angiographic approach provides limited coverage because each acquisition is restricted to one slice, although multiple acquisitions can be combined. However, when using an exogenous contrast agent, it is impractical to apply multiple 2D acquisitions, because each requires its own administration of contrast. To extend coverage, a 3D acquisition is used to image a contiguous volume during a single acquisition. Just as two dimensions of k-space are required to represent a 2D spatial slice, similarly three dimensions of k-space are required to represent a 3D volume (see Fig. 20-1). The 3D gradient-recalled echo (GRE) pulse sequence comprises a slab selection pulse (as opposed to a slice selection pulse), a frequency encoding gradient (which is formed by the gradient echo maneuver), a phase encoding gradient, and a slice encoding gradient that is not present in 2D imaging (see Fig. 20-2). The nature of phase encoding gradients is that they are applied multiple times to encode each dimension of k-space. Therefore, because the 3D acquisition requires two separate phase encoding gradients, the acquisition time is inherently long. Consider a 3D acquisition with the following parameters:
Repetition time (TR) 8 milliseconds
256 Frequency encoding points
128 Phase encoding points
64 Slice encoding points
Scan time = 8 × 128 × 64 = 66 seconds
CONTRAST MECHANISM
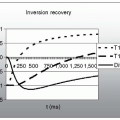
To perform body angiography, a contrast agent is administered through an intravenous line as a bolus, and is followed by a saline flush to ensure that the agent enters the vasculature. The contrast agent reduces the T1 of the blood as it comes in contact with it. When using a short TR imaging sequence with a relatively high radiofrequency (RF) flip angle, the images become T1 weighted. Under these conditions, tissues that have short T1 relaxation times contribute the highest signals, which in this case would be blood. To obtain optimal contrast, it is important to image the contrast agent during its arterial phase. By waiting too long, venous contamination will occur, obscuring the arterial system. However, because contrast transfers from the arterial to the venous system in 15 to 20 seconds, it is imperative to reduce the 3D acquisition time <1 minute (see Fig. 20-3). This can be partially accomplished by the use of a reduce scan matrix. Consider the following modified 3D acquisition parameters:
TR 8 milliseconds
256 frequency encoding points
128 phase encoding points
32 slice encoding points
Scan time = 8 × 128 × 32 = 33 seconds
Another approach to reduce the 3D scan time is to perform centric coding. In this scheme, instead of sampling a full k-space matrix, only the central region is sampled, typically in the shape of an ellipse (see Fig. 20-4). However, this may lead to further reduction in resolution.
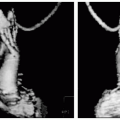
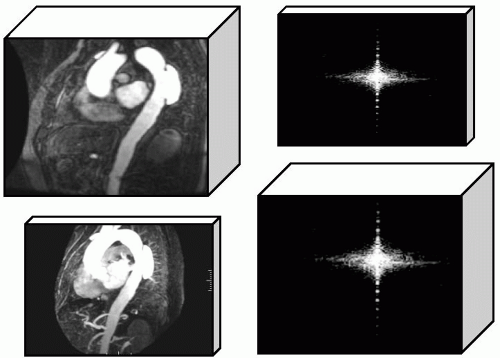 FIGURE 20-1 A two-dimensional (2D) image only provides limited information concerning a thin slice of the body, whereas the vasculature is inherently a 3D structure. The right panel shows the corresponding k-space matrices, that is, a 2D image is formed from a 2D k-space matrix, and a 3D image is formed from a 3D k-space matrix. |
BOLUS INJECTION
A bolus of gadolinium contrast agent is rapidly introduced using a power injector, which employs a dual syringe system. Because optimal contrast is reliant on precisely timing (to within a second or two) the arrival of the contrast bolus with the imaging sequence, bolus administration is under programmable control from the operator’s console. Optimal contrast is also reliant on correct dosage of the agent, which is calculated on the basis of several factors: the extent of the body region to be imaged, the particular contrast agent used, and the imaging purpose. Formulas are used to calculate half dosage (for perfusion), single dosage (for 3D angiography of one region) and double dosage (for 3D angiography of two or more regions).
IMAGE CONTRAST AND K-SPACE
Image contrast is largely determined by the contrast conditions that pertain for lines acquired near the center of k-space. In contrast angiography, we arrange for the central k-space lines to be acquired during the time interval corresponding to peak contrast conditions as the agent traverses the vascular system. Because there is a fairly wide (˜30 seconds) passage time for the contrast agent, it is important to know when the center of k-space is being acquired during this extended acquisition time (see Fig. 20-5). There is varying scanner terminology to indicate when the center of k-space is scheduled to be sampled, for example:
Centric—the k-space center is sampled at the start of the acquisition
Reverse-centric—the k-space center is sampled at the end of the acquisition
Additionally, to determine when to start the acquisition relative to the bolus injection, a “timing sequence” is used:
Inject a small amount of contrast agent.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree