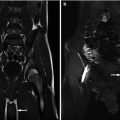
Fig. 20.1
Right adrenal hematoma and right Grade II renal injury in an 8-year-old boy pedestrian in a car struck by a train. CT scan of the abdomen (a) demonstrates shattered spleen, right adrenal hematoma (arrowhead), and (b) superficial laceration of the right kidney. In addition there was large hemoperitoneum
Adrenal injuries are believed to be a result of direct compression and increase in venous pressure caused by compression of the inferior vena cava (IVC). The vascular anatomy of the adrenal gland causes any increase in pressure in the adrenal vein to be immediately transferred to small venules, which cannot accommodate the rapid pressure increase resulting in rupture. It is hypothesized that the short right adrenal vein poorly accommodates (compared to the left adrenal vein) a rapid rise in pressure caused by traumatic compression of the IVC, thus resulting in the predominance of right-sided adrenal injuries [3, 4].
Adrenal injuries are almost exclusively diagnosed by CT scan [3]. The most common finding is an oval or rounded enlarged adrenal gland (Fig. 20.1). Other findings on CT include hematoma that obscures the adrenal outline, stranding of the periadrenal fat, and hemorrhage in adjacent retroperitoneum [3, 4, 7]. A unilateral adrenal injury is typically of minimal clinical significance. In a series of 41 pediatric patients, none required endovascular or surgical intervention for their adrenal [3]. Even the pediatric patients with isolated adrenal injuries (no other injuries identified during trauma evaluation) did not require intervention. Rarely is adrenal replacement required, but clinicians should maintain high suspicion in patients with bilateral adrenal injuries.
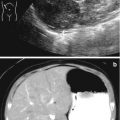
Neonatal adrenal hemorrhage may result from birth trauma and increased abdominal pressure and is associated with ischemia and septicemia (Fig. 20.2). The incidence of neonatal adrenal hemorrhage is 0.2–3 % of live births [8]. The typical presentation is the presence of an abdominal mass and anemia and/or jaundice due to reabsorption of the hematoma, although many children are asymptomatic and there are rare cases complicated with hypovolemic shock due to anemia. Diagnosis is primarily made by ultrasound, which shows a well-defined complex cystic enlargement of the adrenal. The other main possible diagnosis is neuroblastoma. Follow-up imaging is indicated to confirm its involution.
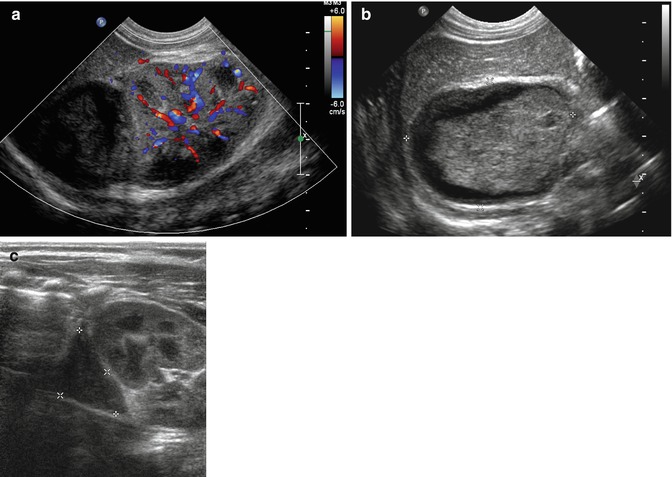
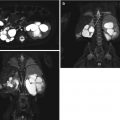
Fig. 20.2
Neonatal adrenal hemorrhage in a large for gestational age term infant post vacuum-assisted vaginal delivery who presented with jaundice, anemia, and suspicion of right renal mass on physical examination. (a) Longitudinal Doppler US demonstrates avascular suprarenal mass with a maximal diameter of 4.4 cm (b). The mass is better delineated on high-resolution linear transducer and demonstrates a well-defined rounded shape with complex fluid. (c) Follow-up US demonstrates marked decrease of the suprarenal mass with a maximal diameter of 2.4 cm, compatible with evolving adrenal hemorrhage
Kidney
The kidney is the most frequently injured genitourinary organ, typically as a result of blunt trauma and present in 2–3 % of all pediatric trauma-related injuries. The pediatric kidney is at increased susceptibility to trauma secondary to multiple anatomic protective factors: softer rib cage, less mature torso musculature, proportionally larger kidneys extending below the protection of the rib cage, and less cushioning perinephric fat [9]. There has been a steady shift over the past 30 years toward conservative therapy for renal trauma, with intervention reserved only for selected patients. Multiorgan trauma is common and present in 50–80 % of patients with any renal injury [10, 11].
Congenitally abnormal kidneys are more susceptible to trauma. Unrecognized renal anomalies are far more common in children and are present in approximately 10 % of children with renal injuries (Figs. 20.3 and 20.4). The most common congenital abnormalities associated with trauma are hydronephrosis, horseshoe kidney, and renal ectopia [12–14]. Despite making the kidney more prone to injury, there does not appear to be an increase in morbidity or mortality [15, 16].
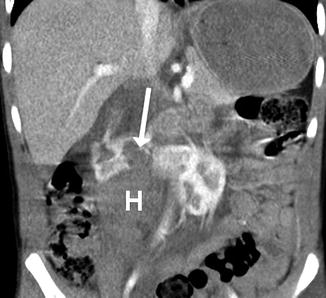
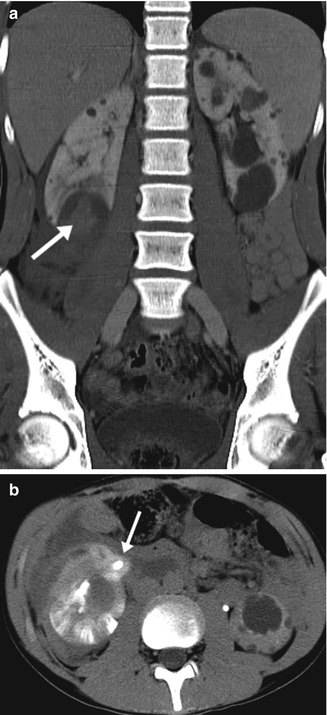
Fig. 20.3
A Grade III renal injury in a 7-year-old boy with a horseshoe kidney who had handlebar injury from a bike. Coronal post-early IV contrast CT scan demonstrates the laceration (arrow) and perirenal hematoma (H)
Fig. 20.4
A right Grade IV renal injury in a 14-year-old who had football injury. (a) Coronal post-early IV contrast discovered bilateral polycystic renal disease with laceration in the lower pole and hematoma in a right lower pole cyst (arrow). (b) Axial post-delayed IV contrast demonstrates contrast extravasation (arrow)
Since the late 1980s CT scan has become the imaging modality of choice for the initial evaluation of suspected renal trauma. CT allows for assessment of injury to the renal parenchyma and hilum, extent of renal hemorrhage, extravasation of urine, as well as associated injuries to other abdominal organs and vasculature structures.
The American Association for the Surgery of Trauma (AAST) has developed a universally accepted grading scale (I–V) to quantify the severity of renal trauma and the likelihood of surgical intervention (Fig. 20.5). There is no consensus on an imaging algorithm for the evaluation of the pediatric trauma patients [17]. The most comprehensive and most algorithm was proposed by McAninch in 2004 and based on observation and management of 374 pediatric patients [18]. This algorithm utilizes the etiology of blunt or penetrating trauma, stability of patient, coupled with the number of red blood cells (RBCs) found on urinalysis (UA) to determine if abdominal CT scan is warranted. They concluded that Abdominal CT scan should be performed in all stable patients with penetrating trauma who have greater than five RBCs on UA and selectively in stable patients with blunt abdominal trauma greater than 50 RBC on UA. The selection criteria to obtain a abdominal CT scan in patients with blunt abdominal trauma, include positive clinical findings of renal trauma (e.g., flank pain, ecchymosis) and rapid deceleration injury. Management of unstable patients depends on the expertise of the medical center. In level 1 trauma center more patients are treated with conservative or minimally invasive procedures (e.g., angiographic embolization, nephrostomy, ureteral stent) as compared to abdominal exploration and nephrectomy. This approach results in a sensitivity for detecting Grade II or greater injuries in over 98 % of blunt trauma and greater than 95 % of penetrating trauma [18]. However, the yield of abdominal CT scan in pediatric patients with microscopic hematuria is very small, and its use should be considered carefully in these patients [19].
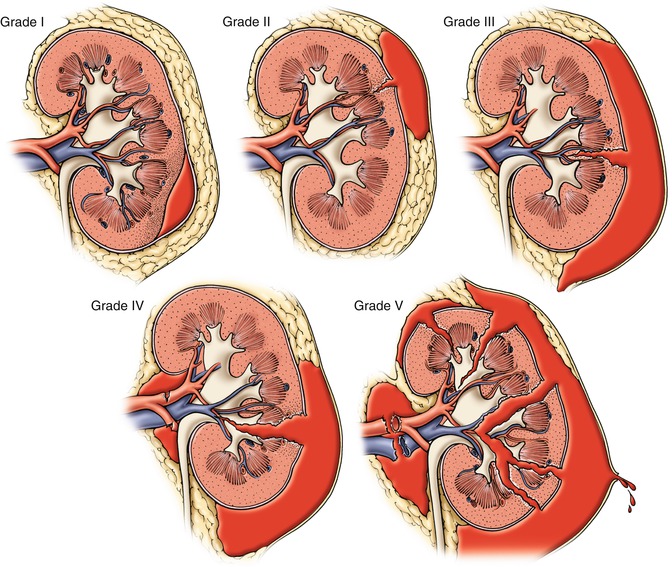
Fig. 20.5
American Association for the Surgery of Trauma (AAST) organ injury scaling for kidney injury, Grade I–V (From Vanni and Wessells [51], www.acssurgery.com. Reprinted with permission. Copyright Decker Publishing)
Some groups have raised concerns that this approach (CT scan for microscopic hematuria >5 RBC/hpf) results in the performance of many unnecessary CT scans which have no impact on clinical course. These groups support the use of established adult trauma criteria for CT scan in the pediatric population; i.e., CT scan is reserved for patients with gross hematuria or are that are clinically unstable [19, 20]. A study simulating this approach in 27 children with microscopic hematuria after blunt trauma showed that only one patient had a Grade IV injury; the kidney was found to be uninjured at surgery [11] and in retrospect misdiagnosed by CT scan.
Ultrasonography (US) evaluation for renal injuries is enticing, as it does not require radiation and can be performed at the bedside, but it lacks sensitivity for detecting solid-organ and vascular injuries. However, if the decision is made to limit CT scanning only to children with gross hematuria, major trauma, or clinical instability, then one may consider use of Doppler US for screening patients with blunt abdominal trauma and microscopic hematuria [19]. At our institution we mainly use US for long-term follow-up of renal injuries.
CT Protocol for Trauma
A single portal venous phase IV contrasts abdominal and pelvis study is performed for any abdominal trauma including for renal trauma. If any renal injury is detected, 5 min delayed CT scan is performed to evaluate for contrast extravasation. To reduce the radiation dose, a split-bolus CT urographic technique has been introduced [21]. It is possible to use three split contrast boluses and scan only once and get all three phases which is our current preference for evaluating vascular, parenchymal, and collecting system injuries (Fig. 20.6) and for follow-up. We use three contrast phases in a single CT scan (Fig. 20.7).
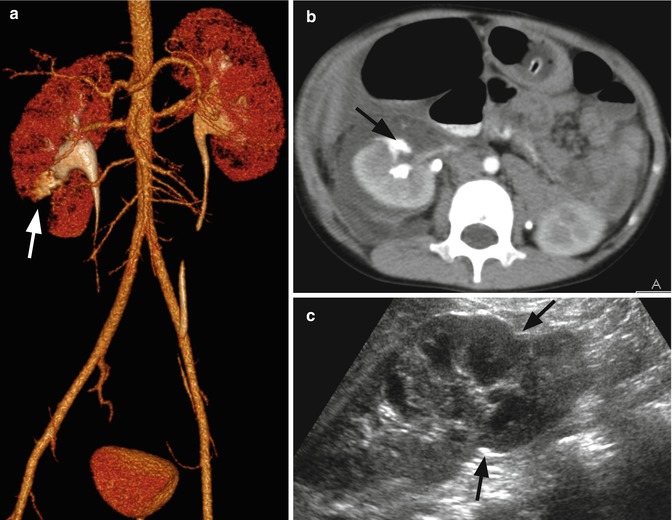
Fig. 20.6
Right Grade IV renal injury in a 5-year-old boy who fell landing on his right flank. He later developed hematuria. Initial CT scan demonstrated Grade IV right renal laceration. A follow-up post-IV contrast CT scan was performed with three-phase technique (arterial, parenchymal, and excretion) in one scan. Volume rendering (a) and axial view demonstrate good opacification of the aorta and major branches including the renal arteries. (b) In the right kidney there is inferior pole triangular-shaped laceration with contrast extravasation (arrows). A 7-month follow-up ultrasound (c) demonstrates lower pole scarring (arrows) and atrophy
Fig. 20.7
Protocol. Contrast volume = 2 mL/kg body weight
1st bolus = 0 s, 20 % contrast volume
2nd bolus = 420 s after the start of the 1st bolus, 35 % of contrast volume
3rd bolus = 60 s after the start of the 2nd bolus, 45 % of contrast volume
Scan after 25 s from the start of the 3rd bolus
Grading
Grade I injuries are defined as hematuria with a normal CT, renal parenchymal contusion, or nonexpanding subcapsular hematoma without parenchymal laceration. This is the least severe renal injury and accounts for approximately 80 % of all renal injuries [18]. Typical CT findings consist of ill-defined or discrete areas of decreased contrast enhancement or with subcapsular hematoma. A subcapsular hematoma is found between the renal capsule and the parenchyma and demonstrates a crescent or elliptical shape, often deforming the parenchyma beneath. A large subcapsular hematoma may cause severe enough compression to impair renal perfusion, resulting in hypertension and a “Page” kidney. Patients with Grade I renal injuries may be observed but frequently do not require admission, bed rest, or any serial laboratory investigations. No follow-up imaging is typically necessary [22–24].
More severe renal injuries occur when the parenchyma tears or splits and include both Grade II and III injuries, determined by depth of laceration. A Grade II injury is defined as either a nonexpanding perirenal hematoma or renal cortical laceration that extends less than one cm (Fig. 20.1). A parenchymal laceration appears as a linear or wedge-shaped defect in the renal enhancement. On CT scan Grade III lacerations extend greater than 1 cm into the renal cortex but do not extend into the collecting system. A perinephric hematoma appears on CT as an ill-defined, high-density fluid collection between renal parenchyma and Gerota’s fascia, rarely deforming the renal contour (Figs. 20.3, 20.8, and 20.9). Throughout multiple series Grade I–III injuries account for over 90 % of all renal injuries and are without question managed conservatively, e.g., bed rest and serial laboratory investigations, and do not often necessitate follow-up imaging nor intervention [22–24].
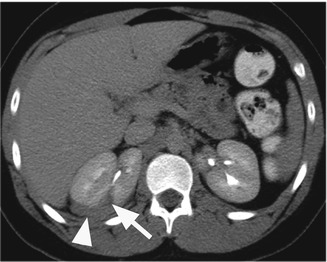
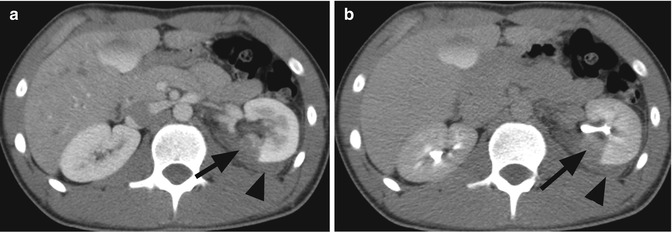
Fig. 20.8
Right Grade III renal injury in a 15-year-old boy stabbed with crooked hook accidentally while playing with his sister at home. Delayed post-contrast CT scan of the abdomen demonstrates a laceration in the right kidney (arrow) with small perirenal hematoma (arrowhead). There is no contrast extravasation
Fig. 20.9
Left Grade III renal injury in a 15-year-old boy with a history of factor IX deficiency who was hit on the left flank during football practice and subsequently began having increased abdominal pain. (a) Initial and (b) delayed post-contrast IV contrast CT scans demonstrated left renal laceration (arrow) with perirenal hematoma (arrowhead). (b) Delayed CT scan did not demonstrate contrast extravasation
Grade IV renal injuries extend through the renal cortex, through the medulla, and into the collecting system, possibly resulting in urinary extravasation. CT delayed phase may show extravasation of urine into the perirenal space (Figs. 20.4, 20.6, and 20.10). Urinary extravasation does not necessitate surgical intervention as over 80 % spontaneously resolve. Follow-up by US can be performed to evaluate change in the extrarenal fluid collection (Fig. 20.9). An injury to the hilum, either venous or arterial, is also considered a Grade IV renal injury. Grade IV injuries including thrombosis, dissection, or injury to the renal vasculature result in segmental infarcts. CT scan may demonstrate active arterial extravasation, which can be managed with angiographic embolization (Fig. 20.10). Infarcts appear as well-circumcised linear or wedge-shaped areas without enhancement.
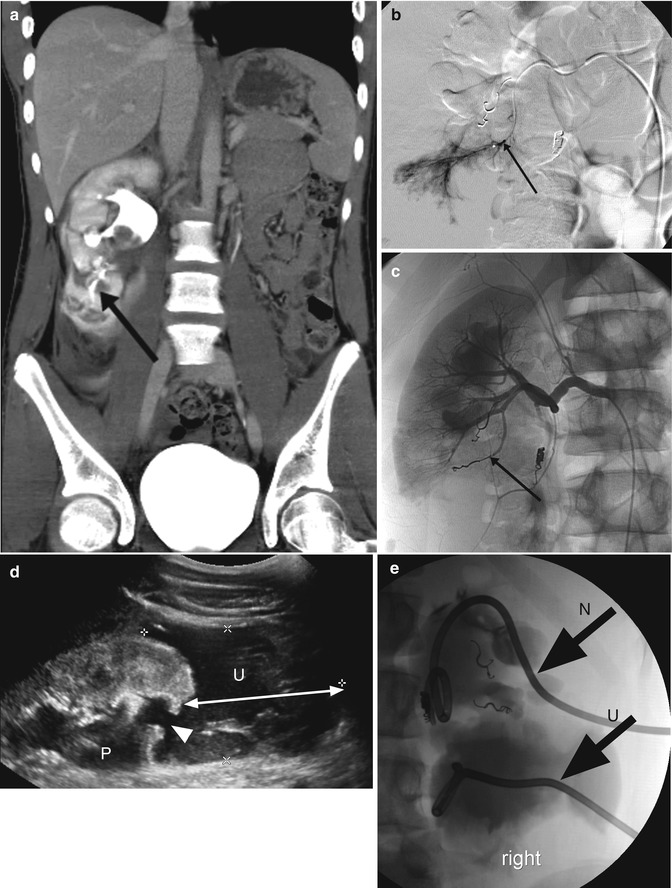
Fig. 20.10
Right Grade IV renal injury in a 15-year-old boy that was crashing into a tree while mountain biking. (a) Post-IV contrast CT scan demonstrates laceration of the lower pole of the right kidney with massive retroperitoneal leak of contrast (contrast in the renal system was secondary to prior outside CT scan). Hemoglobin drop in the second day of admission led to renal angiography study. (b) Selective catheterization of a second-order branch of the lower pole demonstrated small extravasation from terminal arteries (arrow). (c) Three terminal branches were successfully embolized with microcoils. (d) Two-week follow-up ultrasound demonstrated right renal hydronephrosis with moderate dilation of the renal pelvis (P), lower pole laceration (arrowhead), and large (an arrow with two arrowheads) urinoma. (e) Nephrostomy (arrow, N) and pigtail drainage to the urinoma (arrow, U) were placed
Grade IV renal injuries involve any injury to collecting system, including the renal pelvis. Ureteropelvic junction (UPJ) disruption is more commonly seen in pediatric patients, typically resulting from a deceleration injury. A complete UPJ avulsion is diagnosed by lack of contrast in the distal ureter, but a partial UPJ avulsion may demonstrate ureteral contrast. Contrast-laden urine located medial to the renal pelvis and UPJ is often seen in injury to UPJ or the renal pelvis.
Treatment of nonvascular Grade IV renal injury varies, but most can be managed conservatively and will not require intervention. Urinomas may require a ureteral stent or percutaneous drainage in approximately 15 %, while only 10 % require open surgical exploration. One study has shown that medial urinary extravasation on initial CT scan increases risk for necessitating urologic intervention. This same study suggested that lack of filling of the ipsilateral ureter is concerning for UPJ disruption, which likely will require surgical intervention.
Grade V injuries denote a shattered or devascularized kidney or complete avulsion of the renal hilum resulting in devascularization of the kidney. Radiographic appearance of a shattered kidney demonstrates multiple Grade IV injuries, with infarcted, devitalized areas coupled with urinary extravasation secondary to trauma to the collecting system (Fig. 20.11).

Fig. 20.11
Right Grade V renal injury to the upper pole in a 10-year-old girl who fell from a dresser. Axial post-contrast CT scan shows shattered right upper pole (arrow) with a large (arrowheads) retroperitoneal hematoma
Injuries to the renal hilum may not result in hematuria but are almost always associated with significant injuries to other organs. The most common hilar injury is renal artery occlusion secondary to acute stretching of the renal artery causing intimal tearing, arterial dissection, and vessel occlusion. CT will demonstrate a well-defined segment or global absence of renal enhancement but reniform contour is maintained (Figs. 20.12 and 20.13). Right renal artery injuries may also demonstrate retrograde filling of the right renal vein from the inferior vena cava. Collateral perfusion may result in enhancement to the capsule and subcapsular areas, also known as the cortical rim sign, but several hours are required for the appearance of this sign. Isolated renal vein injuries are particularly uncommon, and renal vein thrombosis is often seen in concert with arterial or parenchymal injuries. CT will show renal enlargement, decreased early nephrogram, and prolonged corticomedullary nephrogram with delayed or absent opacification of the collecting system. Laceration of the renal vein demonstrates medial or circumferential subcapsular or perinephric hematoma.

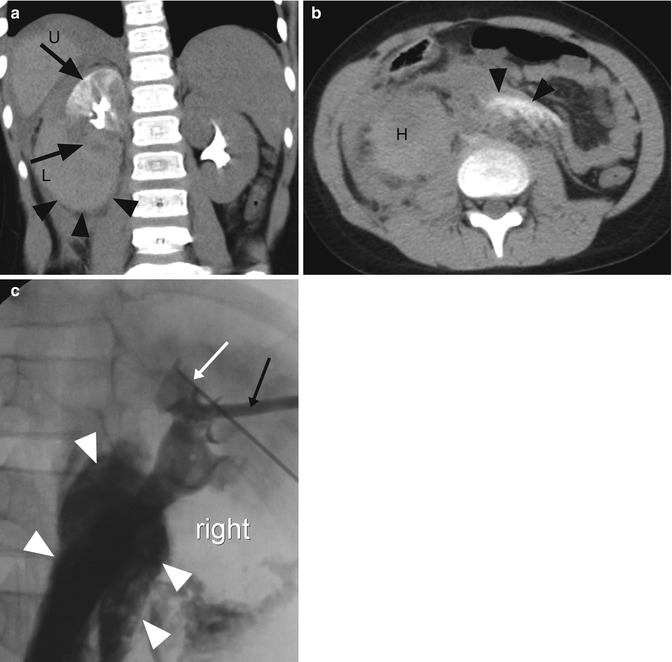
Fig. 20.12
Right Grade V renal trauma, pancreatic and liver lacerations, and severe brain contusion in an 11-year-old boy who had motor vehicle accident. Coronal post-contrast CT scan demonstrates devascularization of the right kidney with active extravasation at the renal pelvis (arrows) and moderate perirenal hematoma (arrowhead). There is large hemoperitoneum and the spleen is devascularized (S)
Fig. 20.13
Right Grade V renal accident to the lower pole in a 7-year-old girl who had sledding accident. (a) Delayed coronal post-contrast CT scan demonstrates devascularization of the lower pole of the right kidney (arrow, L) and large perirenal hematoma (arrowheads). The upper pole (arrow, U) is obstructed with delayed nephrographic phase. (b) Axial delayed post-contrast CT scan at the level of the lower abdomen demonstrates the perirenal hematoma (H) and a central retroperitoneal dense material compatible with contrast extravasation from the collecting system. (c) Nephrostogram was performed using Seldinger technique with 22 gauge Chiba needle (white arrow) and fluoroscopic guidance. An 8.5 French locking drain (black arrow) was placed in the renal pelvis
The management of a Grade V renal injury is complex and should be tailored to each patient, as each individual represents a unique injury. Conservative management is possible in Grade V renal injuries, but often an interventional radiology or surgical intervention is necessary. Follow-up imaging is necessary to assess for expanding hematoma or urinoma. Findings on early follow-up imaging may necessitate percutaneous drains, percutaneous nephrostomy tubes, or ureteral stents for further management. Nephrectomy may be required for unstable patients or unsalvageable renal injuries; however, renorrhaphy should always be attempted prior to nephrectomy.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


