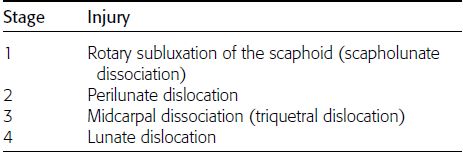
CHAPTER 2 This chapter describes the radiology of many common injuries to the upper extremities in adults. Fractures of the metacarpals and phalanges of the hand are approximately three times more common in men than in women. These injuries have a peak incidence in young men and decrease in incidence with increasing age. Avulsion injuries of the phalanges involve tensile failure of ligamentous or musculotendinous units. These injuries result when excessive loading occurs while the tendon or ligament is already under tension. The substance of a tendon or ligament may tear, or there may be avulsion of its bony insertion. For example, sudden, forcible flexion of the distal interphalangeal (DIP) joint of an extended finger, as occurs when an outstretched finger is struck by a baseball, may result in tensile failure of the extensor mechanism of the distal phalanx. The injury is called a baseball finger, and the resulting clinical deformity is called a mallet finger, in which the DIP joint is maintained in flexion and cannot be extended (Fig. 2.1). An avulsion fracture of the dorsal proximal corner of the distal phalanx is present in 25% of cases of baseball finger; thus, most of these injuries are tendinous. An avulsed bone fragment can be retracted by muscle pull. The converse injury occurs with forcible extension of the DIP joint of a flexed finger or with forcible hyperextension at the DIP joint. In this case, the volar plate of the distal phalanx at the flexor digitorum profundus tendon insertion may be avulsed; alternatively, the tendon may tear. Similar injuries may occur at the proximal interphalangeal (PIP) joint. FIGURE 2.1. Mallet finger resulting from extensor tendon rupture. Purely ligamentous and tendinous injuries are more common than bony avulsions in the fingers, so radiographs may show only soft-tissue swelling or deformities of alignment. Avulsion fractures at the base of a phalanx from the volar edge indicate disruption of the attachment of the volar plate. Avulsions from the lateral edge indicate disruption of the attachments of collateral ligaments (Fig. 2.2). Avulsions from the dorsal edge indicate disruption of the extensor tendon. The avulsed fragments always contain the tendinous or ligamentous insertion (enthesis) and may range in size from a tiny sliver of cortical bone to a large intra-articular fragment. If the intra-articular fragment involves one third or more of the articular surface, the joint may subluxate and require operative fixation. A bony defect should be present where the fragment originated, and although one portion of the fragment has cortex, one portion does not. In contrast to the situation with fracture fragments, accessory ossicles and sesamoid bones invariably are completely corticated, and no donor site should be present. Deformities of alignment reflect the function of the injured unit. In some cases, stress views may be necessary to demonstrate the loss of function. FIGURE 2.2. Avulsion fracture at the collateral ligament insertion of the middle phalanx (arrow). The soft tissues are swollen. The most common dislocation occurs at the PIP joint. Nonmedical personnel often reduce PIP joint dislocations, and many fracture subluxations are actually reduced fracture dislocations. After reduction, if there are no fractures, one may see only soft-tissue swelling. Dorsal dislocations are common, lateral dislocations are less common, and volar dislocations are rare. Fractures involving the phalangeal tufts are the result of direct sharp or blunt trauma. The most common metacarpal fracture is an impacted fracture of the fifth metacarpal neck with volar angulation (boxer’s fracture). It is sustained by bending and axial loading when the closed fist strikes an object (e.g., a wall or chin). In severe cases, the fourth metacarpal neck may also be fractured. Ligamentous disruption of the ulnar collateral ligament of the thumb’s metacarpophalangeal joint, or gamekeeper’s thumb, is sustained during downhill skiing when an improperly planted pole places sudden valgus stress on the thumb. Similar mechanisms of injury may also occur in sports such as football, hockey, wrestling, and basketball. Unless there is an avulsion of a fragment of bone, stress views may be necessary to show this injury on radiographs (Fig. 2.3). On MRI, the torn ulnar collateral ligament may be imaged directly. The adductor pollicis aponeurosis is normally superficial to the ulnar collateral ligament. Interposition of the adductor pollicis aponeurosis between the ruptured ulnar collateral ligament and its distal attachment is called a Stener lesion (Fig. 2.4). A Stener lesion will prevent healing of the ligament and result in chronic instability. FIGURE 2.3. Avulsion fracture (arrow) at the proximal phalanx of the thumb by the ulnar collateral ligament (gamekeeper’s thumb). FIGURE 2.4. Stener lesion. Coronal inversion recovery (A) and coronal T1-weighted MRI (B) show a torn ulnar collateral ligament with proximal retraction (arrow). The adductor pollicis aponeurosis (arrowhead) is interposed between the torn ligament and its distal site of attachment. The exceptional mobility of the thumb in opposing the other digits is possible in part because of a shallow saddle-shaped articulation between the first metacarpal and the trapezium. Axial loading of a partially flexed first metacarpal can produce a simple intra-articular fracture. The adductor pollicis and abductor pollicis longus muscles pull the metacarpal base and shaft proximally, but the anterior lip remains attached to the trapezium by its ligaments (Bennett fracture) (Fig. 2.5). These intra-articular fractures usually require operative reduction and fixation. If a T- or Y-shaped comminuted fracture (Rolando fracture) rather than a simple fracture is sustained, anatomic reduction and fixation may become more problematic (Fig. 2.6). In contrast to these injuries, extra-articular fractures of the first metacarpal shaft present few problems in management because muscle origins along the length of the shaft prevent displacement. FIGURE 2.5. Intra-articular fracture of the base of the first metacarpal with dislocation (Bennett fracture). The small medial fragment (arrow) maintains its attachment to the joint, while the metacarpal has dislocated proximally. FIGURE 2.6. T-shaped fractures (arrow and arrowheads) at the base of the first metacarpal (Rolando fracture) shown by coronal reformatted CT. The wrist positions the hand in space, transmits power to the hand from muscles in the forearm, and transmits mechanical force between the hand and the forearm. Its range of motion is magnified in flexion and extension and in radial and ulnar deviation by a dual articulation: one between the radius and the lunate and one between the lunate and the capitate. With ulnar and radial deviation of the hand, the distal carpal row rotates as well as turns. The carpus can be envisioned as having a central column that consists of the lunate and the capitate. Flexion and extension and the transmission of mechanical force occur through the central column. The capitate, distal carpal row, and hand comprise a single functional unit. The lunate is an intercalated segment between the capitate and the radius that has no direct muscular control (no muscles insert on the lunate). The scaphoid flanks the lunate on one side and functions as a connecting rod alongside the capitate and lunate, providing stability during motion. The triquetrum acts as a pivot for intercarpal rotation through a sloping, helicoid articulation with the hamate. Ligaments of the wrist limit motion when they become taut at their maximum excursion. The volar carpal ligaments are strong and form a sling that suspends the carpus from the radius and triangular fibrocartilage complex (TFCC) (Fig. 2.7). Dorsal ligaments are weaker. Interosseous ligaments bind adjacent carpal bones to each other; those of clinical importance are the scapholunate and lunotriquetral ligaments. The scaphoid and triquetrum flank the lunate on either side and have strong ligamentous attachments to the distal carpal row as well as attachments to the lunate and to the distal forearm. Because no strong ligaments connect the capitate and lunate to each other, the stability of that articulation depends on the integrity of the adjacent scaphoid and triquetrum and their ligamentous attachments. The gap in the volar ligamentous sling at the lunate-capitate articulation is called the space of Poirier. FIGURE 2.7. Ligaments of the wrist. The strong ligaments are on the volar aspect of the wrist and form a sling that suspends the carpus from the distal forearm. The space of Poirier exists because there is no strong ligamentous attachment of capitate to lunate. Many indirect injuries of the carpus involve a carpal sling disruption that extends into the space of Poirier. Radiographic evaluation of the wrist is based primarily on the appearance of each bone and its relationship with the other bones. The arcs made by the proximal articular surfaces of the proximal carpal row, the distal articular surfaces of the proximal carpal row, and the proximal articular surfaces of the distal carpal row are helpful anatomic landmarks. The positions of the scaphoid fat stripe and the pronator quadratus fat pad are occasionally helpful indirect signs of wrist fracture. Scaphoid fractures account for approximately 85% of all isolated carpal bone fractures. The scaphoid bridges the lunate-capitate articulation. With extreme, forceful dorsiflexion between the lunate and the capitate and perhaps the impingement of the scaphoid on the dorsal radial rim, the scaphoid starts to bend, and the fracture line begins on its volar aspect under tensile loading, propagating transversely through the narrowest region (the scaphoid waist). Most scaphoid fractures have no comminution (70% of cases). Less common are fractures through the proximal (10%) or distal (20%) poles. The scaphoid may also fracture during perilunate injuries (discussed later in this chapter). Many scaphoid fractures are nondisplaced and difficult to recognize without special scaphoid views (Fig. 2.8). Indirect signs of scaphoid fracture are obscuration or lateral displacement of the scaphoid fat stripe and soft-tissue swelling over the dorsum of the wrist. Sometimes, it is worthwhile for the radiologist to examine the patient directly. MRI or CT may demonstrate radiographically occult fractures of the scaphoid and other carpal bones (Fig. 2.9). Because the blood supply to the proximal pole of the scaphoid enters the distal pole and courses proximally across the waist, posttraumatic osteonecrosis of the proximal pole with nonunion is a common complication seen in up to 30% of cases. Osteonecrosis of the scaphoid may be directly imaged with MRI. The ultimate prognosis of complicated scaphoid fractures after surgical intervention is favorable. Wrist instability is a common sequela of scaphoid nonunion. FIGURE 2.8. Scaphoid waist fracture. A: The fracture is not visible on the standard PA radiograph. B: Special scaphoid radiograph shows the fracture (arrow). FIGURE 2.9. Radiographically occult scaphoid waist fracture (arrow) demonstrated on T1-weighted MRI. Isolated fractures of carpal bones other than the scaphoid are relatively uncommon. Isolated triquetral fractures usually involve the dorsal surface and are seen best on lateral or slightly oblique radiographs (Fig. 2.10). Isolated lunate fractures usually involve the dorsal or volar surface and are ligamentous avulsions. Pisiform fractures may occur with direct trauma and are best seen on oblique radiographs. Hamate fractures may involve any part, but fractures of the hook of the hamate become displaced by the insertion of the transverse carpal ligament. These may follow falls or direct trauma from the handle of a racquet, golf club, or baseball bat. Complications include nonunion, osteonecrosis, and ulnar or median nerve injury, and most are treated surgically. Dorsal fracture dislocations may also occur at the articulation of the hamate with the bases of the fourth and fifth metacarpals (Fig. 2.11). FIGURE 2.10. Triquetral fracture. Lateral radiograph shows displaced avulsion fragment (arrow) with overlying soft-tissue swelling. FIGURE 2.11. Fracture dislocation of the hamate. A: Radiograph shows dorsal fracture dislocation (arrow) involving the articulations of the fourth and fifth metacarpals with the hamate. B: Axial CT scan shows the displaced, comminuted hamate fracture (arrow). A consistent pattern of injuries is sustained around the lunate when the hand is extended to break a backward fall. On impact, the hand and wrist undergo hyperextension, ulnar deviation, and intercarpal supination (rotary motion between the proximal and distal carpal rows). The ligamentous sling of the carpus is loaded in tension from the radial side, and a sequence of injuries may ensue (Table 2.1). In stage 1, scapholunate dissociation or rotary subluxation, there is rupture of the proximal ligamentous attachments of the scaphoid, opening the space of Poirier on the radial side. The separation of the scaphoid from the middle column leaves scapholunate dissociation. Disruption of the ligaments of the scaphoid allows it to rotate about its short axis in a volar direction (Fig. 2.12). This mechanism of loading may also fracture the scaphoid. In stage 2, perilunate dislocation, the capitate dislocates from the lunate dorsally, taking with it the hand and the scaphoid (Fig. 2.13). The space of Poirier opens on the radial side, often through a scaphoid fracture between the ligamentous attachments to the capitate and lunate, but the triquetral ligaments remain intact. In stage 3, midcarpal dissociation or triquetral dislocation, under continued loading, the triquetral ligaments fail by tear or avulsion of insertions, separating the triquetrum from the lunate. Although the lunate remains in place, the rest of the carpus is dislocated dorsally, coming to rest on the dorsal surface of the lunate. The lunate is subluxated and tilted volarly but is not completely dislocated (Fig. 2.14). Lunate dislocation (stage 4) occurs if there is sufficient force to tear the dorsal radiocarpal ligament, allowing the dorsally dislocated carpus to eject the lunate from the radius volarly. The capitate comes to rest in the radial articular surface. The dislocated lunate is also rotated 90 degrees volarly, still held to the radius by its volar ligaments (Fig. 2.15). Avulsion fractures instead of ligamentous ruptures may occur, including avulsion and tension fractures of the carpal bones (especially the scaphoid) and of the distal radius and ulna. The radiographic signs of reduced perilunate injuries may be subtle, particularly in the absence of bony involvement. TABLE 2.1 Perilunate Injuries of the Wrist FIGURE 2.12. Rotary subluxation of scaphoid. A: Lateral radiograph shows volar rotary subluxation of the scaphoid. The scapholunate angle is nearly 90 degrees. B: PA radiograph shows foreshortening of the scaphoid with a cortical ring sign over its distal pole. C: Scapholunate angle measurement. Normal SL angle is 30 to 60 degrees. FIGURE 2.13. Transscaphoid perilunate dislocation. A: Lateral radiograph shows complete dorsal dislocation of the capitate with normal location of the lunate. B: PA radiograph shows the overlap of the scaphoid and capitate but not the triquetrum. The scaphoid is fractured. FIGURE 2.14. Midcarpal dislocation. A: Lateral radiograph shows complete dorsal dislocation of the capitate and volar subluxation of the lunate. B: PA radiograph shows separation of the scaphoid, capitate, and triquetrum from the lunate. Avulsion fractures of the triquetrum and radial styloid are present. FIGURE 2.15. Lunate dislocation. A: Lateral radiograph shows volar dislocation of the lunate with 90 degrees rotary displacement. The capitate occupies the normal position of the lunate. B: PA radiograph shows the lunate as an overlapping triangular structure. The TFCC is a biconcave fibrocartilage disk interposed between the proximal carpal row and the ulna and suspended by dorsal and volar radioulnar ligaments that extend from the medial aspect of the distal radius to the ulnar styloid process. The TFCC extends the articular surface of the distal radius across the distal ulna, separating the radiocarpal compartment of the wrist from the distal radioulnar joint. Tears of the TFCC may be traumatic or degenerative. Most tears occur through the central portion of the disk where it is thinnest, leading to ulnar-sided wrist pain (Fig. 2.16). Tears that involve the radioulnar ligaments may result in instability of the distal radioulnar joint. Disruption of other carpal ligaments on the ulnar side of the wrist may occur with or without injury to the TFCC. The mechanism and classification of these injuries are not well established. FIGURE 2.16. Central TFCC tear (arrow) shown on T1-weighted fat-suppressed MR arthrogram. The seriousness of ligamentous injuries of the wrist is often overlooked during the acute clinical presentation, particularly if fractures are absent and dislocations have been reduced. When untreated, patients with “wrist sprains” often return with chronic, disabling wrist symptoms, including instability, pain, decreased grip strength, posttraumatic arthritis, and painful “clicks.” Fractures of the distal radius may be associated with more serious carpal dysfunction that becomes apparent once the radial fractures have healed. When the normal wrist is held in neutral position, the axes of the radius, lunate, and capitate are collinear on lateral radiographs. With flexion or extension, approximately half the motion occurs between the lunate and the radius and half between the capitate and the lunate. In dorsiflexion instability (also called dorsal intercalated segment instability, or DISI), the axes of the radius, lunate, and capitate assume a zigzag configuration with dorsal angulation of the lunate (relative to the radius) and volar angulation of the capitate (relative to the lunate). Dorsiflexion instability may be associated with rotary subluxation of the scaphoid but more often follows an impacted distal radius fracture. In volar flexion instability (also called volar intercalated segment instability, or VISI), the zigzag is the reverse, with volar angulation of the lunate (relative to the radius) and dorsal angulation of the capitate (relative to the lunate) (Fig. 2.17). Scapholunate dissociation (rotary subluxation of the scaphoid) may be found following an episode of trauma or in the setting of arthritis. MRI, wrist arthrography, or stress radiographs may be required to document carpal instability or the underlying ligamentous injuries. FIGURE 2.17. Carpal instability patterns on sagittal CT reformations. (R, radius; C, capitate; D, dorsal aspect; V, volar aspect). A: DISI with capitate subluxation. The lunate (arrow) is tilted dorsally. B: VISI. The lunate (arrow) is tilted volarly.
Trauma in Adults: Upper Extremity

 HAND
HAND
Fingers


Thumb



 WRIST
WRIST
Biomechanics
Scaphoid Fractures


Other Isolated Carpal Fractures


Perilunate Injuries








Triangular Fibrocartilage Complex and Ulnar-Sided Injuries
Carpal Instability
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


