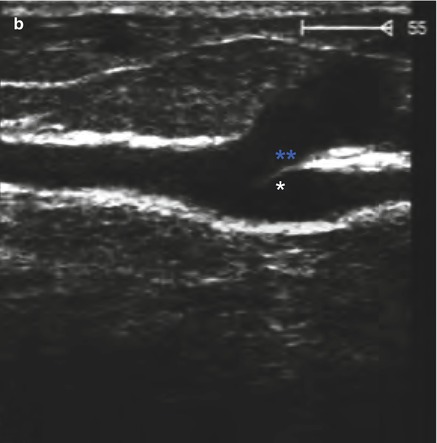
Fig. 10.1
(a) Transverse view through the inner thigh. A small-calibre competent great saphenous vein (GSV) is seen surrounded by its fascial compartment. There is a larger refluxive tributary running superficial to the great saphenous vein and its fascia. The PW curve of the tributary demonstrates relatively more reflux (peak) than antegrade flow (trough). (b) Longitudinal view of a distal to the point where the tributary branches off the great saphenous vein. A visible valve cusp is seen just below the branch point before the great saphenous vein continues footwards. The great saphenous vein is thick walled and surrounded by fascia (**), whereas the tributary has no discernible wall
Copyright: [Author]
10.3.1 Healthy Tributaries
The following tributaries should be examined routinely, even if they are healthy. These are the anterior and posterior accessory saphenous veins, which are automatically included in the examination of the junction and upper section of the great saphenous vein; the posterior arch vein, along which lie the perforating veins which are frequently pathologically dilated; and the upward extension of the small saphenous vein (vein of Giacomini or femoropopliteal vein). The latter, together with the posterior accessory saphenous vein, forms a connection between the great and small saphenous veins. The significance of this is shown in Sect. 10.5.
The above named tributaries can carry pathologically increased blood volumes to the saphenous veins, generally as exclusive reflux sources, but sometimes in addition to incompetent subterminal valves. If this is not diagnosed correctly and the saphenofemoral junction is simply ligated, then the patient will be incorrectly treated because the reflux source will remain. Early clinical recurrence is inevitable with persistence of the patient’s symptoms.
10.3.2 Refluxive Tributaries
Refluxive varicose tributaries are the cosmetic problem for patients. An ultrasound examination of the saphenous veins will identify their refluxive tributaries (Sects. 7.4 and 8.4). The course of the saphenous trunks and all visibly refluxive tributaries are examined also for additional reflux sources.
Refluxive tributaries are sometimes not clearly visible in B scan, because they lie very close under the skin or form large convolutions where the flow on colour duplex is confusing (Fig. 10.2). It is not usually necessary to examine a varicosity down to its detail. However, it is important to establish where the refluxive blood comes from and where it drains by analysing the direction of flow and tracing this carefully with the probe. Identification of the reflux sources and drainage points is arguably the most common skill required in the ultrasound investigation of varicose veins.
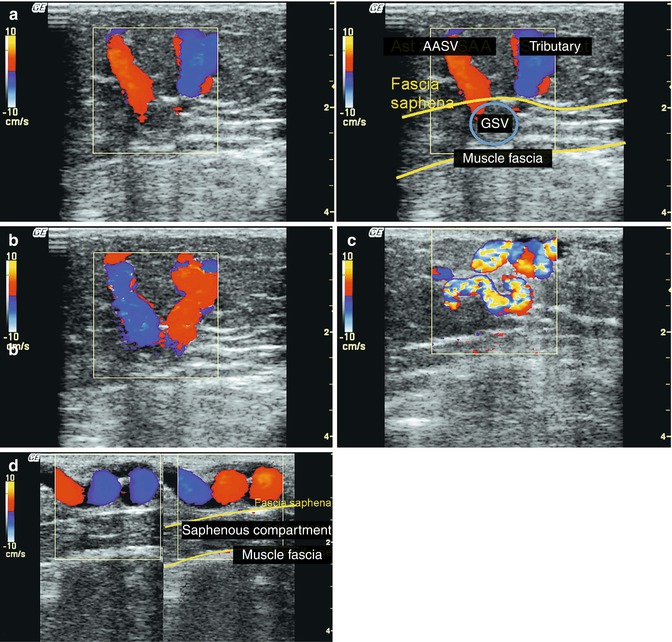
Fig. 10.2
Transverse view from the inner aspect of the right thigh demonstrating a refluxive anterior accessory saphenous vein (AASV) filling a great saphenous vein (GSV) from the lateral side, which is competent proximally and distally. Opposite, a medial tributary is seen refluxing out of the great saphenous vein. (a) Muscular systole; the blood flows upwards in the anterior accessory saphenous vein, towards the probe (red) and downwards from the medial tributary (blue). (b) Muscular diastole; the flow directions are reversed. The refluxive anterior accessory saphenous vein now fills the great saphenous vein which is inwards (blue), and the refluxive tributary carries the blood back to the surface (red) (see accompanying online material). (c) Refluxive tributary in the thigh. Turbulent flow is seen due to the multiple changes of direction in the vessel. The exact flow direction is difficult to determine. It is important to visualise whether there is a connection to the deep vein in this region like a high perforating vein of the adductor canal (formerly Dodd). (d) Longitudinal view of the inner thigh demonstrating a refluxive tributary in systole (left) and diastole (right). Confused colours are apparent due to the many changes in blood flow direction through the convolution
Copyright: [Author]
The net flow direction in tributaries may reveal whether they are secondary varicose veins after deep venous occlusion. It may also determine the extent in which they contribute to the venous return (Chap. 15).
10.3.2.1 Important Drainage Points
The search for the inflow and drainage points of a varicose vein is difficult and tedious. The following technique can help by using either the CW probe or the duplex ultrasound probe in PW or colour mode. First, the probe is placed at the upper end of the vein to be examined. Next, the subject is told to raise and lower his toes (Wunstorf manoeuvre). In this way, reflux can be confirmed in this vein segment. Then the segment below the varicose vein is compressed with one finger and the subject is again asked to activate the muscle pump. If there is no drainage point between the probe and the point of digital compression, no reflux occurs in the first phase of muscular diastole. However, after the digital compression is released (top two curves, Fig. 10.3), reflux will resume. If a refluxive tributary branches off between the middle and lowest compression point Fig. 10.3, the waveform changes. With digital compression at the lowest point, the reflux begins at the onset of muscular diastole which is independent of digital compression. This is because the refluxive volume is now drained by a tributary (bottom curve).
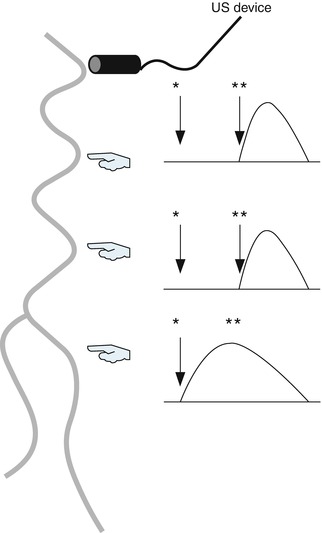
Fig. 10.3
Diagram of the examination technique used to determine the site of important drainage points. The probe is placed at the upper end and the hands indicate the points at which the vein is compressed with the finger. The curve on the right shows the velocity profile in each case after muscle contraction (raising the toes). * beginning of muscular diastole (lowering the toes), ** release of digital compression (see explanation in text)
Copyright: [Author]
10.3.2.2 Important Reflux Source Points
Sometimes it is not obvious which vein is feeding a refluxive tributary. It is helpful in these cases to place the probe on the relevant segment, switch on colour duplex mode and tap the vein further up with one finger of the other hand or run it over the skin. If there is a reflux source further up, then a signal will be recorded in the vein.
10.4 Anterior Accessory Saphenous Vein
The anterior accessory saphenous vein joins the great saphenous vein in the region of the saphenofemoral junction. Rarely, it joins the common femoral vein directly (Fig. 10.4; see also Sect. 7.3.7). It courses downwards lateral to the great saphenous vein. Its first part is in the fascial compartment where it may lie in the same compartment as the great saphenous vein (Fig. 10.5a) or be separated from it by a layer of connective tissue (Fig. 10.5b).
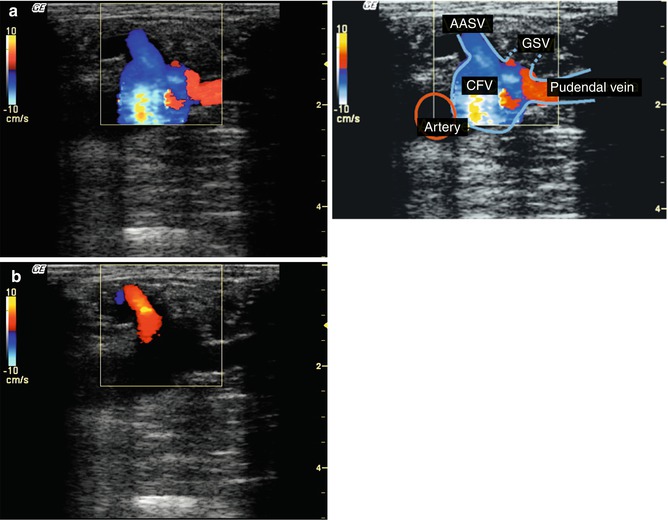
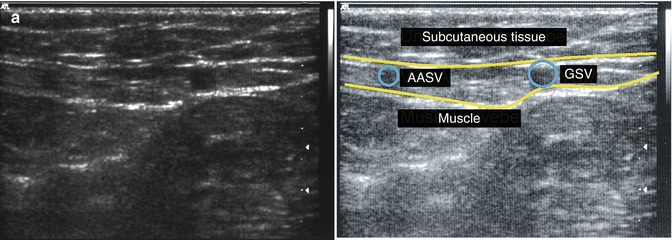
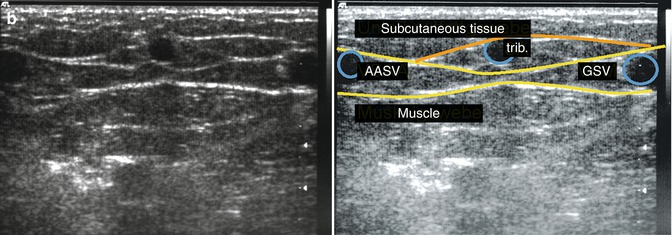
Fig. 10.4
(a) Transverse view through the right groin during muscular systole. Antegrade flow is seen in all the veins. The dilated pudendal vein carries blood towards the probe and therefore appears red. In this case, the junction between the pudendal vein and great saphenous vein is towards the probe, which is the reason it appears red. As the flow is only during systole and not diastole (see b), the pudendal vein is competent, even though it is dilated. The great saphenous vein joins around 2 mm further down. (b) Muscular diastole demonstrating reflux from the common femoral vein directly into the anterior accessory saphenous vein (see accompanying online material)
Copyright: [Author]
Fig. 10.5
Fascial compartment of the anterior accessory saphenous vein. (a) Transverse view through the right thigh 5 cm below the saphenofemoral junction. The great saphenous vein (GSV) and anterior accessory saphenous vein (AASV) are in the same fascial compartment (see accompanying online material). (b) Transverse view through the right thigh 10 cm below the saphenofemoral junction in a different leg. The great saphenous vein and anterior accessory saphenous vein have their own fascial compartments. In the middle of the image, there is a tributary which runs from the anterior accessory saphenous vein to the great saphenous vein where it has left the fascial compartment. However, it remains beneath a fascial remnant (orange)
Copyright: [Author]
After 15–20 cm of coursing interfascially, the anterior accessory saphenous vein usually surfaces from this compartment to follow the midline of the thigh. This configuration is relatively constant. A communicating vein often branches off the anterior accessory saphenous vein, connecting it to the great saphenous vein in this region.
If the anterior accessory saphenous vein is incompetent and filled refluxively from the common femoral vein through an incompetent terminal valve and competent preterminal valve, this communicating vein may carry the reflux further down the great saphenous vein causing it to become incompetent once more. This means that the great saphenous vein can have more than one incompetent segment separated by competent segments (Sect. 4.1.2.3).
On the other hand, only the lower part of the anterior accessory may be affected by reflux. This may occur in patients with reflux of the great saphenous vein to the thigh or an incompetent perforating vein of the adductor canal (formerly Dodd or Hunter). These provide reflux sources to the communicating vein which may fill the anterior accessory saphenous vein refluxively further down the leg. For this reason, the anterior accessory saphenous vein, regardless of whether or not its origin is competent, should always be examined throughout its course.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


