Fig. 4.1
The recirculation circuit. Veins with antegrade flow are shown in blue, refluxive superficial veins in red and perforating veins affected by recirculation in violet. The direction of recirculation flow is marked with arrows (PI proximal reflux point, DI distal reflux point, GSV great saphenous vein, SSV small saphenous vein). The recirculation sections are 1 incompetent great saphenous vein, 2 incompetent tributaries, 3 drainage through perforating vein(s) and 4 deep veins
Copyright: [Author]
First Section
Extends from the proximal to the distal reflux point and therefore consists of the refluxive section of the great saphenous vein. The proximal reflux source is the point where the saphenous vein starts to fill refluxively. It is the highest reflux point in the saphenous vein (Fig. 4.1). The distal reflux point is where the refluxive flow of blood leaves the saphenous vein. Distal to this point, the great saphenous vein is competent (Fig. 4.1).
Second Section
In older phlebology studies, it was believed that the blood always entered a varicose tributary at the distal reflux point. This is the second section of the recirculation circuit. These tributaries are most often found at the end of the refluxive part of the saphenous vein. They are called incompetent varicose tributaries. However, in duplex studies, this is not always the case because reflux may drain to deep veins through perforators without an intervening refluxive tributary.
Third Section
The blood from the incompetent varicose tributaries flows through the different perforating veins into the deep veins.
Fourth Section
This is where the deep veins complete the circuit. Antegrade flow occurs back to the beginning of the recirculation loop.
Hach distinguished different forms of incompetence on proximal reflux source:
Complete Incompetence
If the reflux passes directly through the saphenofemoral junction, from the common femoral vein into the great saphenous vein or the popliteal vein into the small saphenous vein, the situation is one of complete incompetence (Fig. 4.2). Here the saphenous veins are filled by retrograde flow through an incompetent terminal and preterminal valve.
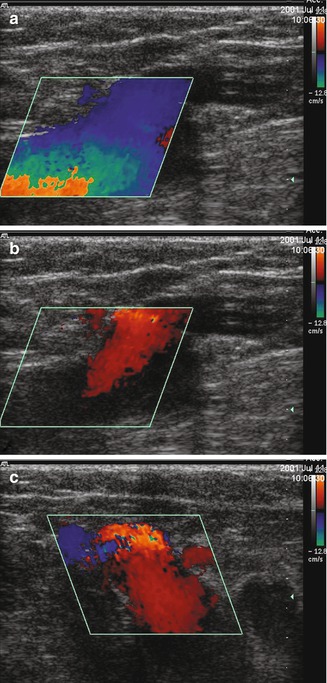
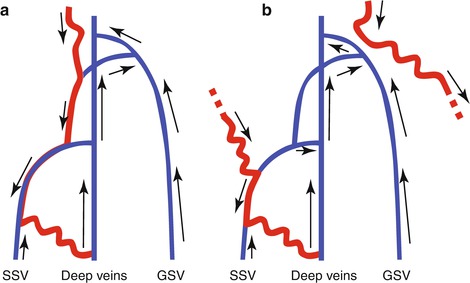
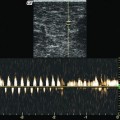
Fig. 4.2
Reflux from the deep veins into a complete incompetence of the great saphenous vein. (a) Longitudinal view through the left groin of a standing patient. The common femoral vein is on the left with the saphenofemoral junction in the centre. During muscular systole, there is antegrade flow in the great saphenous vein, the saphenofemoral junction and the common femoral vein. (b) Identical view 2 s later during muscular diastole. The saphenofemoral junction is refluxive with an incompetent terminal valve. The source of the reflux filling the great saphenous vein is the femoral vein. In the standing patient, blood flows from the femoral vein above the saphenofemoral junction into the great saphenous vein. These findings are similar with a Valsalva manoeuvre. (c) Transverse view through the groin in muscular diastole. There is reflux from the femoral vein through the saphenofemoral junction and into the great saphenous vein. Again, this is similar to the appearances following a Valsalva manoeuvre
Copyright: [Author]
Incomplete Incompetence
If the terminal valve is competent and the saphenous vein fills from another refluxive source, the incompetence is described as incomplete (Fig. 4.3).
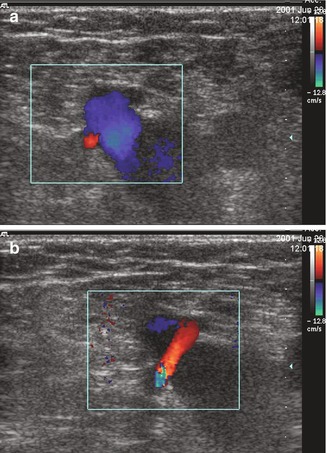
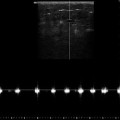
Fig. 4.3
Incomplete incompetence of the great saphenous vein. (a) Transverse view through the left groin. During muscular systole, there is antegrade flow in the great saphenous vein. (b) During muscular diastole, there is no reflux from the femoral vein because the terminal valve is competent. In this case, the pudendal vein is the source of the reflux with retrograde filling of the great saphenous vein
Copyright: [Author]
Hach divided recirculation into compensated and uncompensated. The distinction depends on the condition of the deep veins:
Compensated Recirculation
If the deep leg veins, especially the femoral and the popliteal, are competent and not dilated, then there is compensated recirculation.
Uncompensated Recirculation
If the deep leg veins, especially the femoral and the popliteal, are dilated and incompetent, then there is uncompensated recirculation. In this situation, there is secondary popliteal and femoral vein incompetence.
Secondary incompetence of the deep veins requires a precise definition. A distinction must be made between return flows from deep veins through an incompetent terminal valve into the superficial veins (see Fig. 4.2) and a genuinely incompetent deep vein, with valves which have become secondarily incompetent due to volume overloading.
4.1.2 Great Saphenous Vein
4.1.2.1 First Section, Proximal Reflux Source
Hach distinguishes between complete and incomplete incompetence based on the reflux source. With reflux from the deep veins through the saphenofemoral junction and incompetent terminal valve, the incompetence is complete. With a competent terminal valve and reflux further down the great saphenous vein, the incompetence is incomplete. Depending on the source of the refluxive blood, these are classified into tributary type (55 %), perforating vein type (28 %) when the source of the reflux is from refluxive perforating veins and posterior (dorsal) type (17 %) with a reflux source from the femoropopliteal vein or the posterior accessory saphenous vein.
Based on duplex ultrasound criteria, the reflux source in incomplete incompetence can be differentiated according to:
Reflux source
Course of the reflux into the great saphenous vein bypassing the competent terminal valve
The following are the possible sources of reflux in cases of incomplete incompetence:
Pelvic veins | Pelvic type (see. Fig. 4.4) |
Perforating veins | Perforating type (see Fig. 4.5) |
Small saphenous vein | Small saphenous vein type (see Fig. 4.6) |
Healthy tributaries | Reticular type (see Fig. 4.7) |
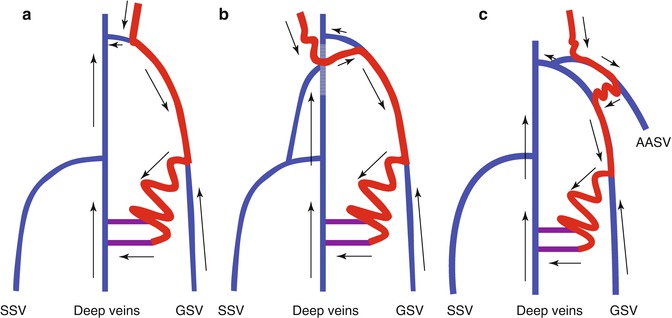
Fig. 4.4
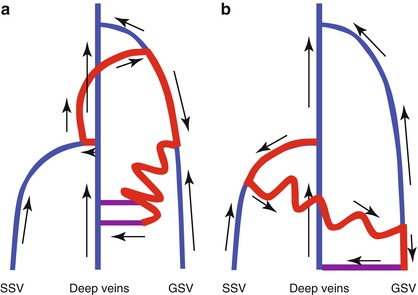
Incomplete incompetence of the pelvic type. (a) Junction tributary type demonstrating reflux from the superficial epigastric vein with a competent saphenofemoral junction, (b) incomplete incompetence of the posterior pelvic type, (c) incomplete incompetence of the anterior pelvic type (AASV anterior accessory saphenous vein, GSV great saphenous vein, SSV small saphenous vein)
Copyright: [Author]
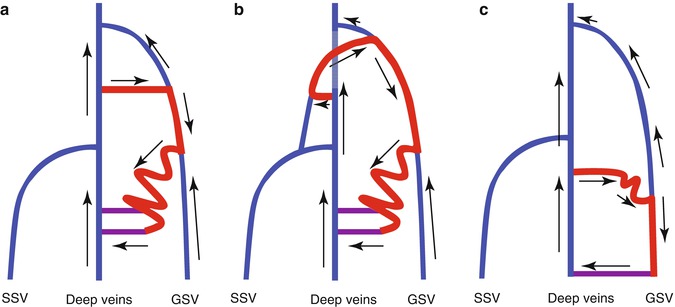
Fig. 4.5
Incomplete incompetence of the perforating type. (a) Direct perforating type demonstrating a direct connection with the perforating vein in the adductor canal (formerly Dodd), (b) posterior perforating type, (c) distal perforating type
Copyright: [Author]
Fig. 4.6
Incomplete incompetence of the small saphenous vein type. (a) Posterior, (b) distal
Copyright: [Author]
Fig. 4.7
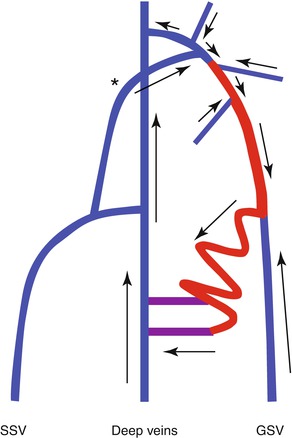
Competent saphenofemoral junction. Antegrade blood from healthy tributaries (blue) and the posterior accessory saphenous vein drains into the great saphenous vein which then refluxes downwards. There is no pathologically refluxive connection with the deep vein system
Copyright: [Author]
Reflux from these sources can reach the great saphenous vein through the following connections:
Direct | Perforating vein in the adductor canal (formerly Dodd, Hunter) or a paratibial perforating vein (Boyd) |
Through a tributary of the saphenofemoral junction | Pelvic type (Fig. 4.4) |
Posterior through the posterior accessory saphenous vein | Pelvic type |
Perforating type (dorsal thigh perforators, formerly Hach perforating vein) | |
Small saphenous vein type through the cranial extension of the small saphenous vein or Giacomini anastomosis | |
Anterior through the anterior accessory saphenous vein | Pelvic type |
Distal through a tributary in the calf | Small saphenous vein type |
Perforating type | |
Through many healthy tributaries in the course of the vein | Reticular type |
4.1.2.2 First Section: Course of the Great Saphenous Vein
In 16.6 % of cases, analysis of refluxing great saphenous veins has revealed that at least one competent segment may exist between two refluxing segments. The competent segment is situated between the proximal and distal reflux point (Mendoza 2002 in Appendix 2). In these cases, the reflux leaves the great saphenous vein by a tributary and re-enters the great saphenous vein further down (Fig. 4.8). This variant is called segmental incompetence. It may occur two or three times along the course of the great saphenous vein.
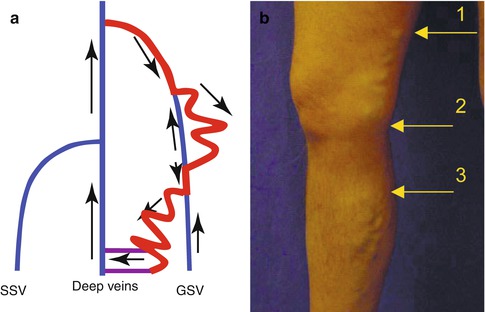
Fig. 4.8
(a) Segmental incompetence of the great saphenous vein with reflux arising initially through the saphenofemoral junction. From there, the reflux enters a tributary in the thigh leaving a competent segment of the great saphenous vein between the knee and the mid thigh. It is then refluxively refilled from the tributary below the knee and then redelivers this reflux to a cluster of varicose veins further down. (b) This situation may be deduced clinically when there are two varicose clusters along the course of the great saphenous vein as seen in the illustration. The great saphenous vein is refluxive above arrow 1, competent between arrows 1 and 2, refluxive between arrows 2 and 3 and competent once more below arrow 3
Copyright: [Author]
4.1.2.3 First Section: Distal Reflux Point
The distal reflux point determines the Hach class (I–IV). This is the point where the reflux leaves the interfascial great saphenous vein and fills a varicose tributary. Alternatively, it may enter the deep veins through a perforating vein. The great saphenous vein distal to this point is competent in its extension down to the ankle (Fig. 4.9):
I | The reflux fills the great saphenous vein and then immediately flows down one of the tributaries of the saphenofemoral junction. The great saphenous vein is therefore refluxive only at the junction region. The reflux then leaves the great saphenous vein in the groin where it remains competent further down |
II | The distal reflux point is in the thigh. The great saphenous vein is competent in the lower leg |
III | The distal reflux point is below the knee. The reflux leaves the great saphenous vein at some point in the lower leg |
IV | The whole great saphenous vein is refluxive down to the ankle |
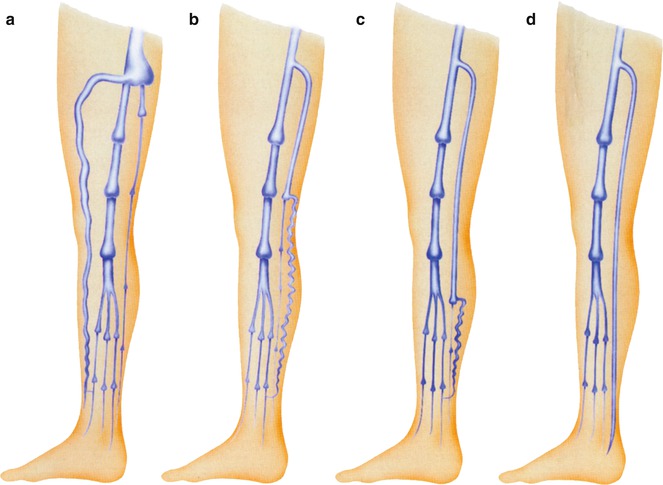
Fig. 4.9
Diagram of the four classes of reflux of the great saphenous vein according to the location of the distal reflux point (source). (a) Distal reflux source within an abnormally dilated termination of the great saphenous vein. In this example, the distal reflux point is the termination of the anterior accessory saphenous vein (Hach I). (b) Distal reflux source in the thigh region (Hach II). (c) In the lower leg (Hach III). (d) In the foot (Hach IV) (From Hach and Hach-Wunderle 1994 in Appendix 2)
Copyright: Springer
The frequency of the various classes has been investigated by Hach using phlebography (Table 4.1, left) and by Mendoza using duplex ultrasound (Table 4.1, right). The latter was from an evaluation in 547 legs with complete saphenous incompetence from an incompetent terminal valve.
Table 4.1
Frequencies of the Hach classes established by phlebography and ultrasound
Hach class | Frequency using phlebography (%) | Frequency using duplex ultrasound (%) |
|---|---|---|
I | 30 | 6.5 |
II | 30 | 22.5 |
III | 40 | 43.4 |
IV | <1 | 1 |
Recognition of the refluxive great saphenous vein from a refluxive tributary may be difficult. Therefore, the following criteria may help to define the distal reflux point:
The refluxive great saphenous vein runs a straight classic course in the fascial compartment where the “saphenous eye” is visible in transverse view (Fig. 7.32).
The refluxive tributary is often tortuous until it pierces the fascia and connects with the great saphenous vein.
Distal from this point, the great saphenous vein is not refluxive and may have a sudden reduction in calibre on the ultrasound image (Fig. 7.34).
The tributary is not protected by a fascia. It remains epifascial throughout its downward course.
The distal reflux point established using the duplex ultrasound criteria given above is sufficient to determine the Hach class for a report to the primary physician and for a general evaluation. Additional information on the course of the great saphenous vein is only relevant for planning treatment.
4.1.2.4 Second Section
The second recirculation section relates to the incompetent varicose tributaries. It is described by Hach but not yet divided into classes. The morphology and presence of tributaries may have influence on the treatment of saphenous vein incompetence. Their removal has been shown by some authors to render competence in saphenous trunks (Pittaluga et al. 2009; Zamboni et al. 2010).
The second component of recirculation is not always apparent. Reflux may flow directly from the first section (saphenous vein) to the third (perforating vein). If incompetent varicose tributaries exist, they are often at the distal reflux point. If there is complete incompetence of the great saphenous vein with reflux to below-the-knee draining through the paratibial perforating vein (formerly Boyd), then a varicose tributary may be found in the thigh (Fig. 4.10). Sometimes the incompetence of the great saphenous vein does not end with the passage of the blood from the great saphenous vein to the tributary in the thigh. It may continue down the great saphenous vein beyond the visible incompetent tributary. In this case, the drainage through the perforator defines the Hach class.
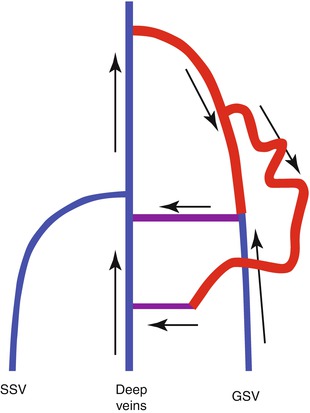
Fig. 4.10
Complete incompetence of the great saphenous vein in Hach class III. The reflux fills an incompetent tributary in the thigh. The great saphenous vein is refluxive to the paratibial perforating vein (formerly Boyd), where the reflux flows into the deep system
Copyright: [Author]
4.1.2.5 Third Section
The re-entry perforating veins comprise the third section. Hach assigns particular significance to the posterior tibial perforating vein (formerly Cockett), without further definition.
The re-entry process is defined as the perforating veins which drain blood from the superficial refluxive veins into the deep veins during muscular diastole (Chap. 9).
In the early stages of venous insufficiency, the perforating vein in the calf serves as a re-entry point for the recirculating blood. As the volume of reflux increases, so does the calibre of the perforating vein.
With a large recirculation volume, the perforating vein becomes very dilated and can no longer be closed by muscular contraction. This causes an outward flow during muscular systole which drains inwards again during muscular diastole (Sects. 3.4 and 9.3.2). This situation can cause dilatation with secondary reflux in the deep veins termed an uncompensated recirculation.
If there is only an outward flow through a perforating vein, then this is either the proximal reflux source or secondary to a deep venous obstruction caused by the post-thrombotic syndrome (PTS). In either case, the perforating vein does not form the third component of the recirculation circuit. Secondary varicose veins caused by the post-thrombotic syndrome are rarely part of a recirculation.
4.1.2.6 Fourth Section
The deep leg veins comprise the fourth section of the recirculation circuit. The blood recirculating through the incompetent superficial veins must be transported by the deep veins in addition to its native blood flow. If there is a large recirculation volume, the veins become dilated to form secondary deep venous incompetence (see Chap. 14).
4.1.3 Small Saphenous Vein
The same principles apply as for the great saphenous vein. There are four sections, with proximal and distal reflux sources in the first section.
4.1.3.1 First Section: Proximal Reflux Source
As described above, complete and incomplete incompetence may be defined on the type of the proximal reflux source. Complete forms of recirculation are those in which the reflux from the popliteal vein enters the small saphenous vein through an incompetent terminal valve (see also Sect. 2.5.1 and Fig. 2.31a–d).
Incomplete incompetence occurs when the reflux source bypasses the competent terminal valve of the small saphenous vein and enters further down. The possible reflux sources correspond to those described for the great saphenous vein.
Under the assumption that the saphenopopliteal junction is competent and that the small saphenous vein is refluxive in its course, the following classification of incomplete incompetence of the small saphenous vein is suggested which is based on the:
Reflux source
Course of reflux into the small saphenous vein bypassing the competent terminal valve
The following are possible original sources of reflux with incomplete incompetence:
Pelvic veins | Pelvic type (see Fig. 4.11) |
Perforating veins | Perforating type (see Fig. 4.12) |
Great saphenous vein | Great saphenous vein type (see Fig. 4.13) |
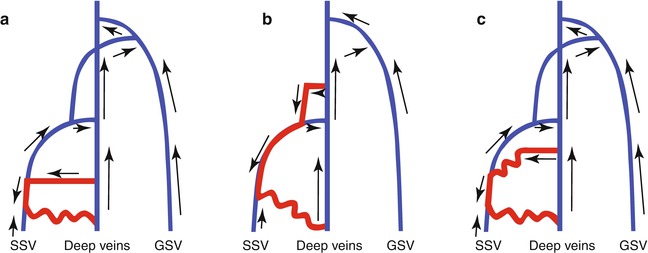
Fig. 4.11
Incomplete incompetence of the small saphenous vein of the pelvic type. (a) In the posterior pelvic type, the reflux from the pelvis flows down through veins on the inner side of the thigh and labia to meet the posterior accessory saphenous vein. (b) In the lateral pelvic type, the reflux from the pelvis flows down through veins in the anterior part of the thigh to meet the anterior accessory saphenous vein. This winds around the lateral side of the leg (interrupted line to the right and re-entering the illustration from the left) to fill the small saphenous vein
Copyright: [Author]
Fig. 4.12
 Examination of Superficial Veins in the Presence of Deep Venous Disease
Examination of Superficial Veins in the Presence of Deep Venous Disease
 Duplex Ultrasound Examination of Superficial Leg Veins
Duplex Ultrasound Examination of Superficial Leg Veins
 Flow Provocation Manoeuvres for the Diagnosis of Venous Disease Using Duplex Ultrasound
Flow Provocation Manoeuvres for the Diagnosis of Venous Disease Using Duplex Ultrasound
 The Ultrasound Scanner
The Ultrasound Scanner
 Examination of the Great Saphenous Vein
Examination of the Great Saphenous Vein
 Anatomy of the Superficial Veins
Anatomy of the Superficial Veins




Related posts:
Examination of Superficial Veins in the Presence of Deep Venous Disease
Duplex Ultrasound Examination of Superficial Leg Veins
Flow Provocation Manoeuvres for the Diagnosis of Venous Disease Using Duplex Ultrasound
The Ultrasound Scanner
Examination of the Great Saphenous Vein
Anatomy of the Superficial Veins
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
