Chapter 117 Overview: Approximately 5% to 10% of children and adolescents with severe hypertension have an underlying renal vascular lesion. In infants, up to 70% of clinically significant hypertension is due to renovascular disease. Myriad developmental and acquired causes of renovascular hypertension exist (Box 117-1). A complication related to umbilical artery catheterization is the most common cause of renovascular hypertension in neonates. In older children, renal arterial fibromuscular dysplasia is the most common cause.1–4 Imaging: Asymmetry of the kidneys on sonography is an important sign of possible renovascular hypertension. The affected kidney often is small and may have manifestations of scarring. Direct visualization of a stenotic renal arterial lesion is uncommon with sonography, however. Evaluation of the aorta also is an important component of the examination. With Doppler evaluation, a renal artery-to-aorta peak systolic velocity ratio of greater than 3.5 carries a strong association with renal arterial stenosis. A peak velocity in the renal artery of greater than 180 cm/s also is suggestive of renal artery stenosis. Distal to the stenotic lesion, the systolic peak of the renal arterial waveform often appears flattened (Fig. 117-1). With severe stenosis, Doppler evaluation of distal arteries shows a tardus-parvus pattern, with slow systolic acceleration and diminished peak systolic velocity. Diastolic flow in the main renal artery sometimes is elevated.5 Figure 117-1 Renal artery stenosis. The most useful scintigraphic technique for detection of renovascular hypertension involves the evaluation of renal function without and with the use of an angiotensin-converting enzyme inhibitor, usually captopril or enalaprilat. MAG3 is the optimal imaging agent for this study. In the presence of renovascular disease, imaging in conjunction with angiotensin-converting enzyme inhibitor therapy typically shows diminished perfusion, diminished initial uptake, and poor parenchyma clearance of the affected kidney. Comparative imaging in the absence of antihypertensive therapy shows improved function (Fig. 117-2). The sensitivity of this technique for the detection of renovascular hypertension is approximately 85% to 90%. Bilateral renal artery stenosis or markedly compromised renal function can lead to false-negative examinations.6 Figure 117-2 Renovascular hypertension and angiotensin-converting enzyme (ACE) inhibition scintigraphy. Transcatheter angiography is the most sensitive and specific technique for the detection and identification of small-vessel renal artery disease. Computed tomographic angiography (CTA) and magnetic resonance angiography (MRA) are important noninvasive techniques for visualization of renal vascular anatomy. Upon administration of contrast material, global and regional alterations in kidney perfusion and function also can be assessed with computed tomography (CT) and magnetic resonance imaging (MRI). In general, >50% narrowing of the renal arterial diameter is hemodynamically significant. The presence of enlarged collateral pathways is an additional indicator of significant renal artery stenosis. Transcatheter renal vein renin sampling is useful in selected cases of suspected renal hypertension (Fig. 117-3).7,8 Figure 117-3 An 11-year-old girl with hypertension. Overview: Renal fibromuscular dysplasia (FMD; arterial fibrous dysplasia) is the most common cause of renal artery stenosis in children. Subcategorization of FMD is based on the layer of the arterial wall that is involved. This classification is important because each type of FMD has distinct histologic and angiographic features and occurs in a different clinical setting.9–11 Primary intimal fibroplasia is characterized by circumferential accumulation of collagen subintimally and within the internal elastic membrane. This form of FMD is the most common cause of renal artery stenosis in children. Imaging shows a smooth, bandlike, tubular, or funnel-shaped stenosis that usually involves the distal two thirds of the renal artery or a branch vessel (Fig. 117-4). Overview: The most common vascular pathology in patients with neurofibromatosis type 1 involves stenosis of the aorta or a large branch vessel as a result of proliferation of neural tissue in the arterial wall and perivascular space. Occasionally, an aneurysm occurs. In the kidney, a small-vessel mesodermal dysplasia also can occur. Arterial stenosis usually occurs at the vessel origin or in the proximal third of the main renal artery. Concomitant aortic stenosis is common.12 Overview: Takayasu arteritis is a rare idiopathic chronic inflammatory arteritis. Hypertension as a result of renal arterial stenosis or abdominal aortic narrowing is common. CT and MRI features of Takayasu arteritis include narrowing, mural thickening, adherent thrombus, and mural calcification of the aorta, pulmonary arteries, and major aortic branch vessels (Fig. 117-5). With active disease, the thickened vascular wall has prominent contrast enhancement.13–15 Overview: Middle aortic syndrome (midaortic dysplastic syndrome) is an acquired, progressive vascular disorder that involves the midthoracic through abdominal segments of the aorta and usually is accompanied by narrowing of major visceral branches, including the renal arteries. Imaging studies show diffuse narrowing of the thoracoabdominal segment of the aorta and the major branch vessels (Figs. 117-6 and 117-7). If renal artery narrowing is severe, collateral flow to the kidneys usually occurs via ureteral, adrenal, and gonadal arteries that fill from lower intercostal vessels.16,17 Figure 117-6 Middle aortic syndrome.
Vascular Conditions
Renovascular Hypertension
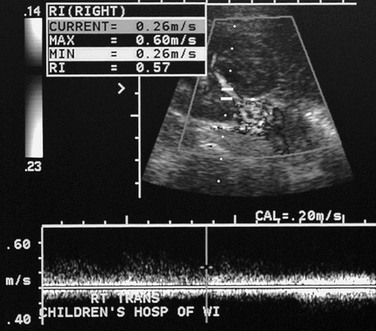
Doppler evaluation of the renal artery distal to a severe stenosis in a child with renal fibromuscular dysplasia shows a low-velocity monophasic arterial waveform.
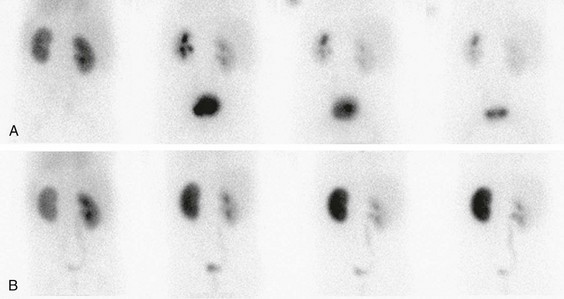
A, A renogram shows normal uptake and excretion from both kidneys. B, A renogram after administration of an ACE inhibitor shows marked radiopharmaceutical retention in the left kidney, indicating renal artery stenosis. (Courtesy Douglas F. Eggli, MD, Hershey, PA.)
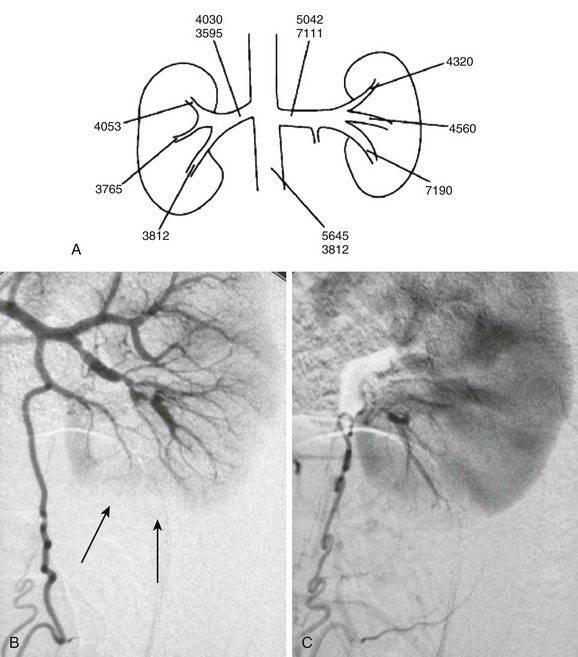
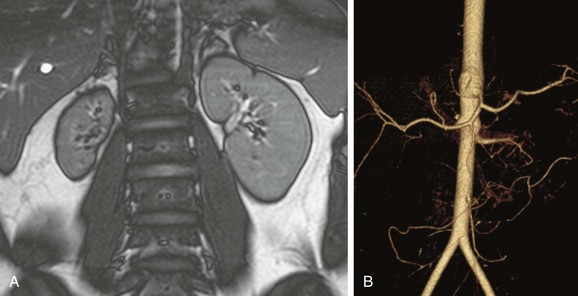
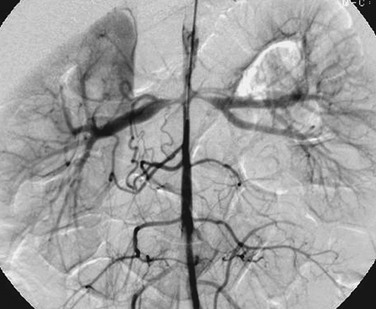
A, A map of renal vein renin activity shows that the hypertension is driven by a focus in the left lower pole. B, Arterial phase angiography shows complex segmental stenoses, an area of delayed perfusion owing to a “missing vessel” (arrows), and a prominent collateral ureteric artery. C, Capillary phase angiography shows that the ureteric artery collateral reconstitutes the “missing vessel,” completing the nephrogram. (From Roebuck DJ. Paediatric interventional radiology. Imaging. 2001;13:302-320.)
Renal Fibromuscular Dysplasia
Neurofibromatosis
Takayasu Arteritis
Middle Aortic Syndrome
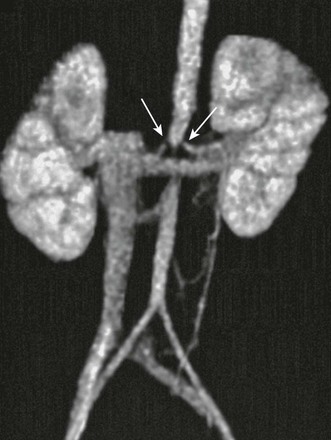
Computed tomographic angiography of a child with middle aortic syndrome reveals severe narrowing of the renal arteries (arrows) and infrarenal portion of the abdominal aorta.
Renovascular Trauma