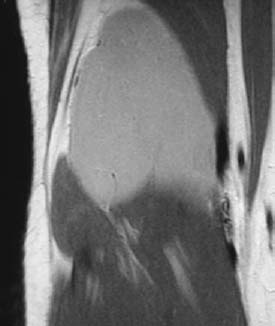
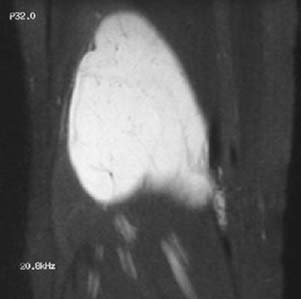
CASE 45 Anthony G. Ryan and Peter L. Munk A 25-year-old woman presented with a large palpable swelling behind her knee. This case was referred to us to rule out a deep venous thrombosis (DVT). Figure 45A Figure 45B A lateral radiograph of the distal thigh (Fig. 45A) shows a lucent soft-tissue swelling posterior to the distal femur. Because of the clinical suspicion of DVT, an ultrasound (Fig. 45B) was performed. It revealed a mixed hyperechoic and hypoechoic lesion superficial to the popliteal neurovascular bundle, thought initially to be cystic, specifically a Baker’s cyst, especially given the presence of posterior acoustic enhancement. No communication with the joint was demonstrable, however, and the patient was subsequently referred for MRI. An axial T2-weighted image (Fig. 45C) seems to confirm the suspicion of a cystic lesion, returning very high signal. However, coronal (Fig. 45D) and sagittal (Fig. 45E) T1-weighted images demonstrate the lesion returns intermediate signal intensity hyperintense to skeletal muscle, which is inconsistent with simple fluid, and several low signal intensity foci consistent with flow voids. Sagittal T1-weighted postintravenous gadolinium (Fig. 45F) and coronal T1-weighted postintravenous gadolinium with fat-saturated (Fig. 45G) images confirm that the lesion is solid, demonstrating intense enhancement throughout. Figure 45D Figure 45E Figure 45F Figure 45G Liposarcoma: myxoid subtype. Liposarcomas are a heterogeneous group of lesions comprising malignant tumors of mesenchymal origin containing variable adipose components. They are the second most common soft-tissue sarcoma in adults after malignant fibrous histiocytoma, comprising 12 to 18% of all malignant soft-tissue sarcomas. They occur most frequently in the fifth and sixth decades and are almost unheard of in the pediatric population. The crucial decisions on imaging are the differentiation of a lipomatous or myxomatous lesion with malignant potential from benign lipomatous or myxomatous lesions, and to stratify those lesions with malignant potential into low-grade (e.g., nonmetastasizing), well-differentiated liposarcoma and high-grade lesions (e.g., the pleomorphic variant), although the final arbiter of this decision is invariably histological. All liposarcomas demonstrate a genetic clonal abnormality resulting in amplification of the 12q13–15 region. Lipomas do not share this genetic lesion, making this one of the criteria used by pathologists to differentiate these entities. Dedifferentiation is thought to occur in roughly 10% of well-differentiated liposarcomas, occurring three times as often in retroperitoneal lesions (15% risk of differentiation) than in extremity lesions (5% risk). This difference is thought to be a result of the longer “time to discovery” for retroperitoneal lesions. As with other sarcomas, hematogenous metastasis to the lungs followed by the visceral organs is the expected pattern. Myxoid liposarcomas have a predilection for metastases to scerosal and pleural surfaces, subcutaneous tissues, and bone. A concomitant mass in the retroperitoneum or thigh may be present in up to 10% of myxoid liposarcomas, presenting as either a multicentric lesion or a primary lesion with a secondary deposit at initial diagnosis. Liposarcomas are subclassified by the World Health Organization into four major subtypes and a fifth subtype comprising a mixture of elements of the other subtypes: Well-differentiated liposarcoma represents the lowest, and dedifferentiated liposarcoma the highest, grades of tumor. There are two distinguishable histologic types sharing cellular pleomorphism:
Liposarcoma
Clinical Presentation


Radiologic Findings


Diagnosis
Differential Diagnosis
Discussion
Background
Etiology
Pathophysiology
Clinical Findings
WELL-DIFFERENTIATED LIPOSARCOMA
MYXOID LIPOSARCOMA
PLEOMORPHIC LIPOSARCOMA
DEDIFFERENTIATED LIPOSARCOMA
MIXED LIPOSARCOMA
Stages of Disease
Complications
Pathology
WELL-DIFFERENTIATED LIPOSARCOMA
Gross
Microscopic
MYXOID LIPOSARCOMA
Gross
Microscopic
PLEOMORPHIC LIPOSARCOMA
Gross
Microscopic
DEDIFFERENTIATED LIPOSARCOMA
Gross
Microscopic

Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


