George M. Bridgeforth, Shane J. Nho, Rachel M. Frank, and Brian J. Cole
A 38-Year-Old Man Who Fell On Outstretched Hand Complains Of Right Shoulder Pain, And He Has Trouble Moving His Shoulder.

CLINICAL POINTS
- A fall on an outstretched hand may injure the AC joint.
- Associated fractures of the wrist, collarbone, scapula, and humerus may be present.
- Patients commonly hold the affected arm adducted at the shoulder, flexed at the elbow, and pronated at the wrist.
Clinical Presentation
Acromioclavicular (AC) joint injuries are relatively common. They are commonly caused by a downward force applied to the AC joint. In the workplace, they can be caused by following objects and falling onto the outstretched hand. In sports, such as hockey or football, they can be caused by hard checks or tackles. AC injuries occur most often in males in the second decade of life.
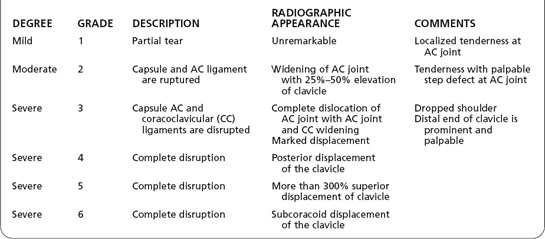
Patients with AC joint injuries often have pain and limited range of motion above the shoulder level (90 degrees), with abduction (raising the forearm outward laterally toward the head) being affected more severely than flexion (raising the forearm in front of the body toward the head). Injuries can be classified as follows (Table 32.1):
- Grade 1: point tenderness at the AC joint but no pronounced dislocation
- Grade 2: moderate pain and soreness with a mild step off
- Grade 3: moderate–to-severe pain and soreness but with a more prominent step-off
- Grade 4: severe pain; marked but unusual deformity in which the clavicle is pushed behind the AC joint
- Grade 5: severe pain; end of clavicle punctures muscle above the AC joint, causing a significant bump
- Grade 6: very pronounced and rare cosmetic deformity in which the clavicle is pushed downward
During the patient assessment, it is necessary to perform a thorough evaluation of the patient. The clinician should
- Rule out a fracture to the clavicle, humerus, or scapula.
- Rule out head or cervical trauma. Patients with C5 radiculopathies may complain of pain or numbness that radiates from the cervical region to the lateral shoulder. To help diagnose acute cervical radiculopathy, the examiner should perform a Spurling’s test by placing downward (axial) force on the head while rotating the head and tilting it laterally. Patient complaint of radicular symptoms is a positive test. Note that patients with unstable cervical injuries are not candidates for a Spurling’s test.
- Always check the lower extremities for upper motor neuron signs (spasticity, hyperreflexia, upgoing plantar responses [positive Babinski test]) for all cervical injuries. The presence of bilateral upper motor neuron signs in a patient with cervical trauma is indicative of spinal cord damage at the cervical region (e.g., severe central cervical stenosis).
- Suspect an accompanying pneumothorax in any patient with direct shoulder trauma who complains of shortness of breath. It is necessary to perform a cardiovascular examination to rule out a pneumothorax, especially with high-impact injuries. Be wary of associated chest trauma. With any bruising of the chest wall and shortness of breath, obtain two-view chest radiographs and rib films of the affected area.
- Rule out rotator cuff tears, which may result in pain-limited abduction, such as AC joint injuries. However, rotator cuff tears are usually accompanied by weak external rotation (outward rotation of the forearm away from the body when the elbow is flexed at 90 degrees). Both conditions may lead to pain-limited extension (i.e., when the hand is placed on the lower back), but with an AC injury, the pain is usually localized to the AC joint.
Table 32.1 Acromioclavicular (AC) Joint Injuries
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


