• MR is a good alternative to CT in pregnant patients, and children when US is nondiagnostic
TOP DIFFERENTIAL DIAGNOSES
• Mesenteric adenitis and enteritis
• Ileocolitis
• Crohn disease
• Gynecologic causes
• Cecal diverticulitis
• Appendiceal tumor
• Cecal carcinoma
• Cystic fibrosis
CLINICAL ISSUES
• Clinical diagnosis is incorrect in ∼ 20% of young men and 40% of young women
• Also frequently in error in young children and older adults
(Left) This graphic illustrates some of the characteristic features of acute appendicitis, including the distended, thick-walled, inflamed appendix and inflammatory thickening of the adjacent walls of the cecum and terminal ileum .
(Right) Axial CECT in 12-year-old boy shows perforated appendicitis. Note the appendicolith and cecal wall thickening . The focally necrotic wall of the appendix delineates the point of perforation. Pericecal and periappendiceal inflammatory changes are also evident.
(Left) Longitudinal sonogram demonstrates a distended, thick-walled appendix , 10 mm in diameter with adjacent hyperechoic periappendiceal inflammation of fat , indicative of an inflammatory process and diagnostic for appendicitis.
(Right) Color power Doppler sonography in a patient with acute appendicitis demonstrates marked hyperemia in the wall of the appendix , indicative of inflammation and consistent with acute appendicitis.
TERMINOLOGY
Definitions
• Acute appendiceal inflammation due to luminal obstruction and superimposed infection
IMAGING
General Features
• Best diagnostic clue
Distended, thick-walled, noncompressible appendix (≥ 7 mm) on US
Abnormal mural enhancement of distended appendix on CECT
Periappendiceal fat stranding on US or CT
• Location
Appendix arises from cecal tip, but tip may lie some distance from cecum
• Size
Noncompressible appendix on US
– > 6 mm has sensitivity of 100%, but specificity of only 64%
– > 7 mm has sensitivity of 94% and specificity of 88%
– 6-7 mm equivocal size; increased flow on color Doppler in appendix indicates positive study
• Morphology
Tip of appendix often 1st site of inflammation and appendiceal perforation
Radiographic Findings
• Radiography
Appendicolith in < 5% of patients (on plain films)
Air-fluid levels within bowel in RLQ
– Due to focal ileus
Loss of right psoas margin
Appendiceal lumen may be patent to point of obstruction
With perforation
– Small bowel obstruction (SBO)
– RLQ extraluminal gas (uncommon to rare)
– Displacement of bowel loops from RLQ
CT Findings
• NECT
Dilated appendix ≥ 7 mm
Periappendiceal fat stranding
Appendicolith
– Seen much more frequently on CT than on radiography
– Even noncalcified appendicoliths may be seen on CT
With perforation
– Small bowel obstruction
– Inflammatory phlegmonous or fluid collections demonstrating mass effect, most commonly in RLQ or dependent pelvis (cul-de-sac)
• CECT
Dilated appendix ≥ 7 mm
– Sensitivity 95%, specificity 95%
Abnormal enhancement of appendiceal wall on CECT
– Inflamed mucosa may show hyperenhancement
– Necrotic wall may show no enhancement
– Wall may be discontinuous at point of perforation
± bubbles of extraluminal gas
Appendicolith may be present (15-40%)
Focal bowel wall thickening of adjacent wall of cecum &/or terminal ileum
– Focal ileus of distal small bowel due to inflammation and spasm of lumen
– Frank SB obstruction may occur with abscess or delayed diagnosis
RLQ extraluminal inflammation
– Diffuse nonencapsulated inflammation of mesoappendix, mesenteric and omental fat (“phlegmon”)









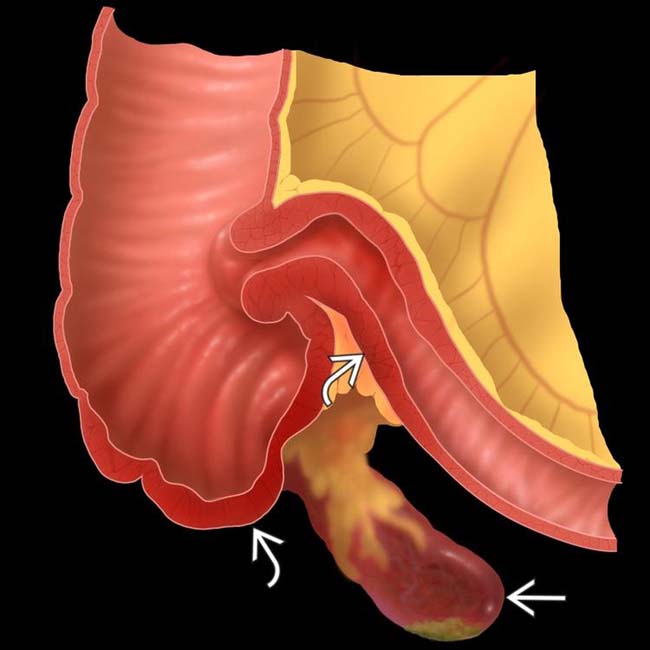
 and inflammatory thickening of the adjacent walls of the cecum and terminal ileum
and inflammatory thickening of the adjacent walls of the cecum and terminal ileum  .
.
 and cecal wall thickening
and cecal wall thickening  . The focally necrotic wall of the appendix
. The focally necrotic wall of the appendix  delineates the point of perforation. Pericecal and periappendiceal inflammatory changes are also evident.
delineates the point of perforation. Pericecal and periappendiceal inflammatory changes are also evident.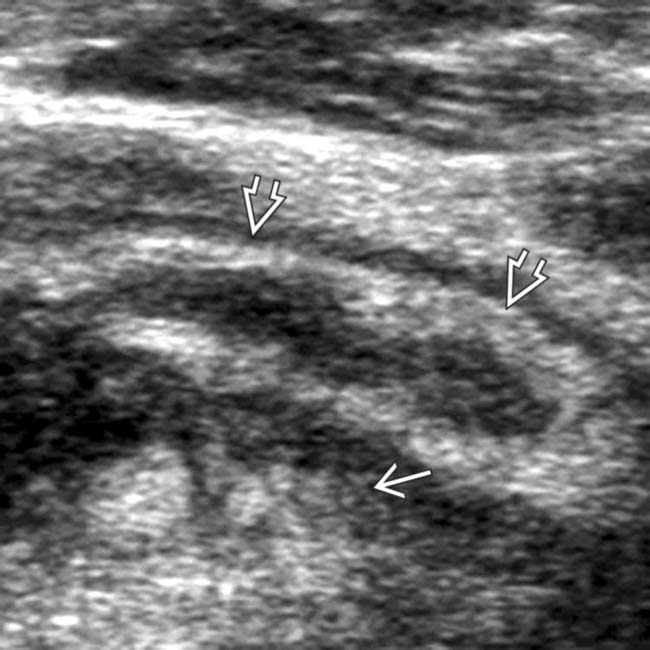
 , 10 mm in diameter with adjacent hyperechoic periappendiceal inflammation of fat
, 10 mm in diameter with adjacent hyperechoic periappendiceal inflammation of fat  , indicative of an inflammatory process and diagnostic for appendicitis.
, indicative of an inflammatory process and diagnostic for appendicitis.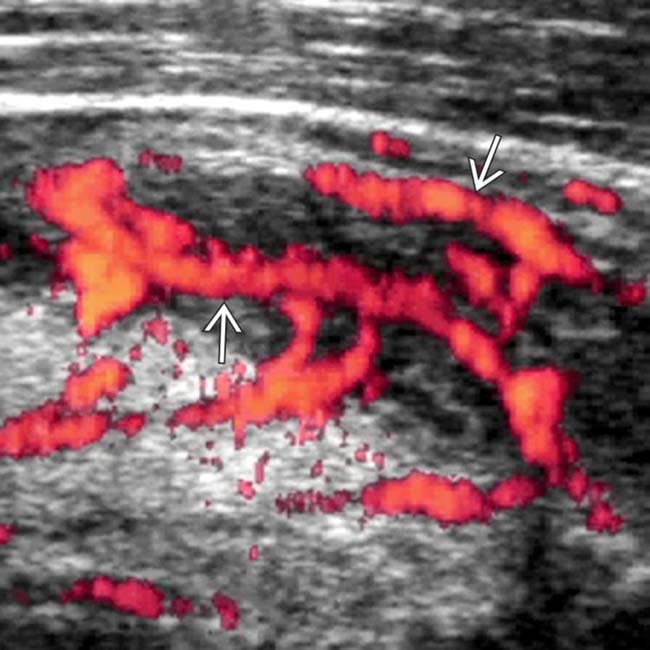
 , indicative of inflammation and consistent with acute appendicitis.
, indicative of inflammation and consistent with acute appendicitis.

























 Noncompressible appendix ≥ 7 mm
Noncompressible appendix ≥ 7 mm





