Large, heterogeneous, moderately enhancing, exophytic mass with necrosis and cystic change
•
Small cell carcinoma
Highly aggressive, with hematologic and lymphatic metastases at time of diagnosis
Large, homogeneous, mildly enhancing mass with confluent local and distant lymphadenopathy
May be indistinguishable from lymphoma
•
Giant cell carcinoma (pleomorphic or osteoclast)
Resection often impossible due to large size
Large, heterogeneous, cystic, low-density mass with frequent hemorrhage, septation, and calcification
•
Acinar cell carcinoma
Slightly better prognosis than adenocarcinoma
Large, well-circumscribed mass with cystic degeneration, exophytic component, and enhancing capsule
Usually no biliary/pancreatic duct dilatation
Vascular occlusion uncommon (20%); may invade the portal vein/superior mesenteric vein
•
Pancreatoblastoma
Most often occurs in children (mean age 2.5 years), but very rarely affects adults (mean age 40 years)
Poor prognosis: Worse outcomes in adults than children
Large, heterogeneous mass with frequent internal calcifications and necrosis/hemorrhage
No pancreatic or biliary duct obstruction
•
Pancreatic plasmacytoma
Consider in patients with known myeloma
Homogeneous mass without pancreatic/biliary ductal obstruction or pancreatic atrophy
Mimics lymphoma, but usually no lymphadenopathy
•
Pancreatic Lipoma
Benign fat-containing mass (-80 to -120 Hounsfield units) with surrounding capsule
Most often occur in pancreatic head
•
Pancreatic schwannoma
Usually benign, with malignant transformation very rare
Well-circumscribed mass ± cystic degeneration
Can closely mimic neuroendocrine tumors (usually with less avid vascularity)
•
Pancreatic adenocarcinoma, pancreatic neuroendocrine tumor, lymphoma, mucinous cystic neoplasm
•
Anaplastic carcinoma: Pleomorphic carcinoma, undifferentiated carcinoma, sarcomatoid carcinoma
•
Small cell carcinoma: Poorly differentiated carcinoma
•
Giant cell carcinoma: Pancreatic osteoclastoma
•
Rare pancreatic malignancies that may mimic adenocarcinomas and neuroendocrine tumors
•
Anaplastic carcinoma
Large, heterogeneous, moderately enhancing, exophytic mass with necrosis and cystic change
Locally invasive with frequent lung and liver metastases
•
Small cell carcinoma
Large, homogeneous, mildly enhancing mass with confluent local and distant lymphadenopathy
May be indistinguishable from lymphoma
Pancreatic head; homogeneous, hypovascular
•
Giant cell carcinoma (pleomorphic or osteoclast)
Large, heterogeneous, cystic, low-density mass with frequent hemorrhage, septation, and calcification
–
Tendency to arise in pancreatic body and tail
–
Often grow to very large sizes (mean > 6 cm)
Local invasion and distant mets (liver, lung) uncommon
•
Acinar cell carcinoma
Large, well-circumscribed mass with cystic and necrotic degeneration and frequent exophytic component
–
Usually a well-defined enhancing capsule
–
Hypodense on both arterial and venous phases
–
Usually no biliary/pancreatic duct dilatation (even with large tumors)
–
Vascular encasement or occlusion uncommon (20%), and may invade portal vein or SMV
Commonly misdiagnosed as neuroendocrine tumor
No predisposition for any specific location in pancreas
Metastasizes to liver and local lymph nodes
•
Pancreatoblastoma
Can resemble either pancreatic adenocarcinoma or neuroendocrine tumors
Associated with Beckwith-Wiedemann and familial adenomatous polyposis










 Most often occurs in children (mean age 2.5 years), but very rarely affects adults (mean age 40 years)
Most often occurs in children (mean age 2.5 years), but very rarely affects adults (mean age 40 years)










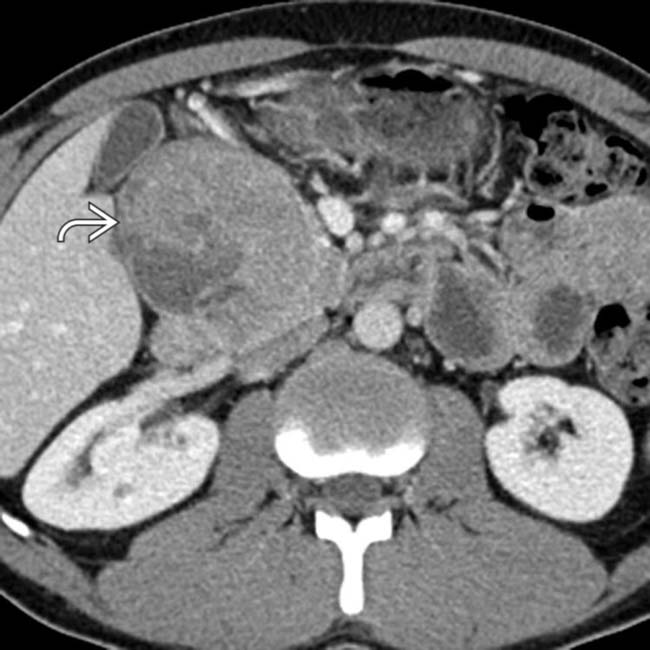
 in the pancreatic head with solid and cystic components. This was found to be an acinar cell carcinoma at surgery. As in this case, these tumors often mimic the appearance of neuroendocrine tumors, albeit with less hyperenhancement.
in the pancreatic head with solid and cystic components. This was found to be an acinar cell carcinoma at surgery. As in this case, these tumors often mimic the appearance of neuroendocrine tumors, albeit with less hyperenhancement.
 arising from the pancreatic tail. This mass was found to be an acinar cell carcinoma at surgery.
arising from the pancreatic tail. This mass was found to be an acinar cell carcinoma at surgery.
 in the pancreatic head.
in the pancreatic head.





 Large, heterogeneous, cystic, low-density mass with frequent hemorrhage, septation, and calcification
Large, heterogeneous, cystic, low-density mass with frequent hemorrhage, septation, and calcification
 Large, well-circumscribed mass with cystic and necrotic degeneration and frequent exophytic component
Large, well-circumscribed mass with cystic and necrotic degeneration and frequent exophytic component


 Large, heterogeneous mass with frequent internal calcifications and necrosis/hemorrhage
Large, heterogeneous mass with frequent internal calcifications and necrosis/hemorrhage







