Left hepatic duct formed by segmental branches from segments II-IV
Right hepatic duct has 2 branches, including a horizontally oriented anterior branch draining segments V and VIII and a vertically oriented posterior branch draining segments VI and VII
Right and left hepatic ducts converge at porta hepatis to form common hepatic duct (CHD)
Cystic duct usually joins CHD just below confluence of right and left hepatic ducts
Only central intrahepatic ducts seen normally (measuring ≤ 3 mm): Visualization of ↑ intrahepatic ducts concerning for dilated ducts or strictures
• Most common variants
Usually aberrant right posterior branch which can drain into left hepatic duct (“crossover anomaly”), CHD, common bile duct (CBD), cystic duct, or gallbladder (GB)
Most frequent: Right posterior duct drains into left duct
2nd most common is right posterior duct fusing with lateral (right) aspect of right anterior duct
TOP DIFFERENTIAL DIAGNOSES
• MRCP artifacts may simulate or obscure pathology
Intraductal mimics of gallstones (gas, flow artifact)
Spasm of sphincter of Oddi
CLINICAL ISSUES
• Normal biliary variants are common (42% of population)
• No clinical significance unless surgery is planned
• Risk of injury if surgeon is unaware (especially anomalies of cystic duct and right hepatic duct)
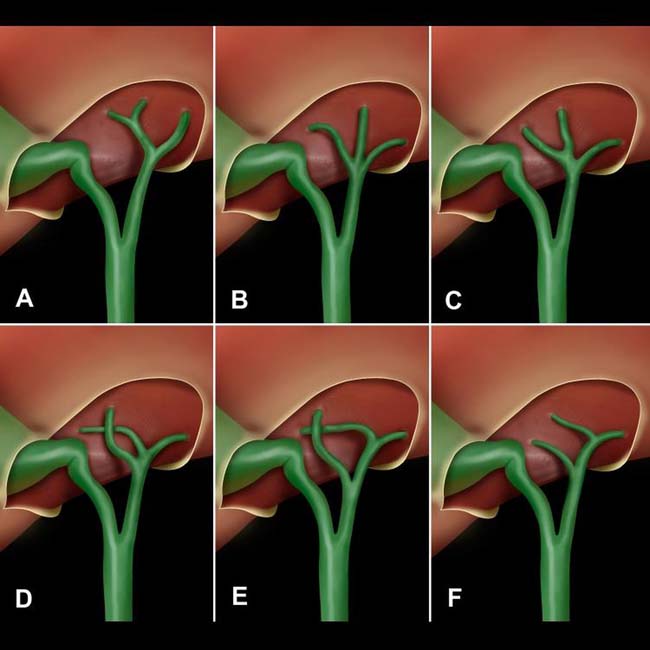
(Left) Upper left-hand graphic (A) shows the conventional arrangement of the bile ducts. Variations are common, especially with aberrant insertion of the right posterior duct, as seen in figures D-F. This may lead to inadvertent ligation or transection at surgery.
(Right) Graphic shows common variations in the course and insertion of the cystic duct, leading to difficulty in isolation and ligation at cholecystectomy. The cystic duct may be mistaken for the common hepatic or common bile duct.
(Left) Intraoperative cholangiogram shows a peculiar bilobed cystic dilation of the distal common duct , presumably a type 3 choledochal cyst or choledochocele. Also noted is aberrant drainage of the posterior lobe bile duct into the common hepatic duct.
(Right) Coronal MRCP with MIP reconstruction demonstrates separate origins of the right anterior and posterior ducts from the common duct. MRCP has a very high concordance with ERCP for identifying biliary tree variants.
TERMINOLOGY
Definitions
• Variants and artifacts that may simulate pathology or potentially complicate hepatobiliary surgical procedures
IMAGING
General Features
• Normal biliary anatomy
Right hepatic duct (which is typically relatively short) has 2 branches
– Anterior (ventrocranial) branch drains segments VI and VIII and has horizontal course extending lateral and towards right from right hepatic duct
– Posterior (dorsocaudal) branch drains segments VI and VII and has vertical course extending upward from right hepatic duct
– Right posterior duct fuses to right anterior duct from medial approach
Left hepatic duct formed by segmental branches from segments II-IV
Bile duct from caudate lobe can join origin of left or right hepatic ducts
Right and left hepatic ducts converge at porta hepatis to form common hepatic duct (CHD)
Cystic duct usually joins CHD just below confluence of right and left hepatic ducts
Only central intrahepatic ducts seen on MRCP in normal patients (≤ 3 mm): Visualization of too many intrahepatic ducts raises concern for ductal strictures or dilatation
• Most common variants
Most common anatomic variants involve aberrant right hepatic duct
– Occurs in > 10% of general population
– Usually aberrant posterior branch, which can drain into left hepatic duct (“crossover anomaly”), CHD, common bile duct (CBD), cystic duct, or gallbladder (GB)
Most frequent is right posterior duct draining into left hepatic duct (13-19% of population)
2nd most common variant is right posterior duct fusing with lateral (right) aspect of right anterior duct (∼ 12% of population)
– May complicate or preclude living donor right liver transplantation
– May result in bile leak or stricture following cholecystectomy
Abnormal junction of hepatic ducts
– Trifurcation pattern (“triple confluence”), with single junction of left hepatic duct with anterior and posterior branches of right hepatic duct (11% of population)
Right hepatic duct nonexistent in this pattern
Accessory hepatic ducts seen in 2% of patients
Anomalous insertion of cystic duct
– Low insertion into common duct (10% of population)
– May insert into right hepatic duct
– May insert into medial aspect of common duct
– May follow parallel course to CHD over several cm
– Must be recognized at cholecystectomy to avoid iatrogenic biliary injuries
• Uncommon or rare variations
Duplication of cystic duct or CBD
Agenesis of GB (rare, ± other anomalies in 75%)
Duplication of GB (very rare)
Cholecystomegaly (enlarged GB)
– Acquired anomaly
– Seen in patients with diabetes, sickle cell disease, or pregnancy, as well as after truncal vagotomy
Microgallbladder
– Acquired, most often in cystic fibrosis patients
• Pancreaticobiliary junction variants
Separate entrance of CBD and main pancreatic duct into duodenum
Long (> 8 mm) common channel of distal CBD and pancreatic duct
CBD may enter side of pancreatic duct
– > 1.5 cm proximal to ampulla of Vater
– Commonly seen in type I choledochal cyst
Only gold members can continue reading. Log In or Register to continue
 Right hepatic duct has 2 branches, including a horizontally oriented anterior branch draining segments V and VIII and a vertically oriented posterior branch draining segments VI and VII
Right hepatic duct has 2 branches, including a horizontally oriented anterior branch draining segments V and VIII and a vertically oriented posterior branch draining segments VI and VII

 Only central intrahepatic ducts seen normally (measuring ≤ 3 mm): Visualization of ↑ intrahepatic ducts concerning for dilated ducts or strictures
Only central intrahepatic ducts seen normally (measuring ≤ 3 mm): Visualization of ↑ intrahepatic ducts concerning for dilated ducts or strictures Usually aberrant right posterior branch which can drain into left hepatic duct (“crossover anomaly”), CHD, common bile duct (CBD), cystic duct, or gallbladder (GB)
Usually aberrant right posterior branch which can drain into left hepatic duct (“crossover anomaly”), CHD, common bile duct (CBD), cystic duct, or gallbladder (GB)











 , presumably a type 3 choledochal cyst or choledochocele. Also noted is aberrant drainage of the posterior lobe bile duct
, presumably a type 3 choledochal cyst or choledochocele. Also noted is aberrant drainage of the posterior lobe bile duct  into the common hepatic duct.
into the common hepatic duct.
 Right hepatic duct (which is typically relatively short) has 2 branches
Right hepatic duct (which is typically relatively short) has 2 branches




 Most common anatomic variants involve aberrant right hepatic duct
Most common anatomic variants involve aberrant right hepatic duct










 CBD may enter side of pancreatic duct
CBD may enter side of pancreatic duct







