Heterogeneous enhancement on arterial phase; usually hypodense on venous and delayed phase CT + MR
Hyperintense on T2W MR
Bright on DWI MR
± capsule, fat, venous invasion, metastases
TOP DIFFERENTIAL DIAGNOSES
• Treated liver metastases or lymphoma
• Budd-Chiari syndrome
• Hepatic sarcoidosis
• Primary portal vein thrombosis
• Nodular regenerative hyperplasia
DIAGNOSTIC CHECKLIST
• MR has advantage in detection and characterization of focal nodules within cirrhotic liver
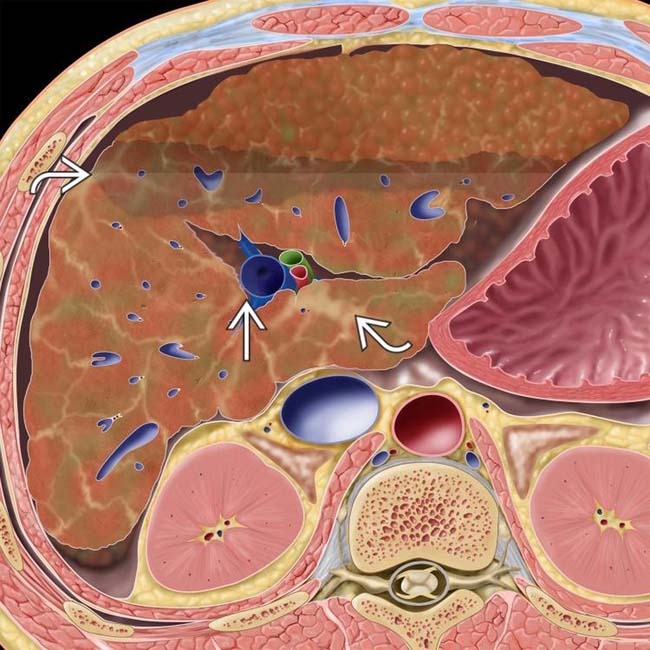
(Left) Graphic shows a cirrhotic liver with a nodular surface contour and an increase in the caudate to right lobe ratio, measured from the branch point of the right portal vein to the edges of the caudate and right lobes, respectively. Note the bands of fibrosis and ascites.
(Right) Axial CECT shows a cirrhotic liver and large varices . Note the enlarged caudate lobe , which is as wide as the right lobe, although the caudate lobe is normally no more than 60% of the width of the right lobe.
(Left) Axial NECT in this 50-year-old woman with primary biliary cirrhosis shows innumerable small hyperdense regenerative nodules , surrounded by lace-like fibrosis.
(Right) The nodules disappear into the background cirrhotic liver on this CECT from the same patient. Prominent porta hepatis lymphadenopathy , another typical feature of primary biliary cirrhosis, is also noted. Primary biliary cirrhosis is an autoimmune disease that typically affects women in their 5th or 6th decade.
TERMINOLOGY
Definitions
• Chronic liver disease characterized by diffuse parenchymal injury, extensive fibrosis, and conversion of liver architecture into structurally abnormal nodules
IMAGING
General Features
• Best diagnostic clue
Nodular contour, widened fissures, and enlarged caudate lobe with ascites, splenomegaly, and varices
• Size
Moderate to advanced cirrhosis: Decreased size
– Earlier disease: May be enlarged
– Especially in primary biliary cirrhosis
• Key concepts
Common end response of liver to variety of insults and injuries
Classification by morphology (not very useful)
– Micronodular (Laennec) cirrhosis
Usually due to alcoholism
– Macronodular (postnecrotic) cirrhosis
Usually viral hepatitis
Classification by etiology and severity more useful
CT Findings
• Atrophy of right lobe and medial segment of left lobe
• Enlarged caudate lobe and lateral segment of left lobe
Caudate: Right lobe ratio often > 1.0 in cirrhosis
Caudate is normally < 60% width of right lobe
• Widened fissures between segments/lobes
• Deep gallbladder (GB) fossa
GB often lies against anterolateral abdominal wall
• Vascular derangements
Varices (gastroesophageal, caput medusae, etc.)
Arterioportal and portovenous shunts
– Arterioportal (AP) shunts are usually peripheral, wedge-shaped, small; seen only on arterial phase
– Small AP shunt difficult to distinguish from very small hepatocellular carcinoma (HCC)
Follow-up imaging (CT or MR) in 3-6 months is sufficient for surveillance
“Corkscrew” hepatic arterial branches
– Enlarged and displaced around regenerative nodules
• Splenomegaly
• Nodular liver contour (not apparent in all)
• Siderotic regenerative nodules
Hyperdense on NECT, isodense on CECT
Most regenerative nodules are not detected by CT
• Fibrotic and fatty changes
Fibrosis: Diffuse, lace-like, thick bands or confluent “masses”
– More apparent on NECT (hypodense)
– May show persistent enhancement on delayed CECT (or contrast-enhanced MR)
Distinguishes from HCC, which shows washout on delayed imaging
Fatty changes: Diffuse or geographic areas of low attenuation
– Usually limited to alcoholic hepatitis with early cirrhosis
• Peribiliary cysts
Cystic dilation of peribiliary gland in wall of large bile ducts
Range in size from 2 mm to 2 cm
Resemble string of pearls or grapes on a stem
• Cirrhosis-induced HCC
NECT: Hypodense or heterogeneous, ± fat
CECT
– Heterogeneous enhancement on arterial phase; usually iso- to hypodense on venous and delayed phase scans
– ± capsule, portal or hepatic venous invasion, metastases
MR Findings
• Siderotic regenerative nodules: Paramagnetic effect of iron within nodules
T1WI: Hypointense
T2WI: Increased conspicuity of low signal intensity
T2 gradient-echo and fast low-angle shot (FLASH) images
– Markedly hypointense (best sequence for detection)
Gamna-Gandy bodies (siderotic nodules in spleen)
– T1WI and T2WI: Hypointense
• Dysplastic regenerative nodules
T1WI: Hyperintense; T2WI: Hypointense
– Opposite to usual pattern for HCC
Minimal vascularity
Take up and retain hepatobiliary MR contrast agents on delayed phase
– Most specific test to distinguish from HCC
• HCC nodule
T1WI: Iso-, hypo-, or hyperintense
T2WI: Hyperintense
T1 C+: Increased enhancement on arterial phase
– Washes out to hypointense on venous and delayed phases
Diffusion-weighted imaging
– Restricted diffusion (bright signal) within HCC
Rarely take up or retain hepatobiliary MR contrast agents
• Fibrotic and fatty changes
T1WI: Fibrosis = hypointense; fat = hyperintense
T2WI: Fibrosis = hyperintense; fat = hypointense
• MR elastography
Shows promise in noninvasive evaluation of extent of liver fibrosis
Ultrasonographic Findings
• Grayscale ultrasound
Nodular liver contour and parenchyma
Increased and coarsened liver echogenicity
– Decreased visualization of deep liver
Atrophy of right lobe and medial segment of left lobe
Features of portal hypertension
– Increased pulsatility of portal vein Doppler tracing
– Dilated hepatic and splenic arteries with increased flow
• Color Doppler
Used to determine portal vein patency and direction of flow
– Hepatopetal is normal
– Hepatofugal is sign of severe portal hypertension
• Ultrasound is of most value and accuracy in screening patients with less advanced chronic liver disease
Less accurate in detecting or characterizing nodules within cirrhotic liver
Presence of fibrosis, fat, regenerative nodules makes detection of HCC very difficult
Imaging Recommendations
• Best imaging tool
Multiphasic CT or MR
• Protocol advice
US is suitable for screening until cirrhosis is established
CECT is preferable in acutely ill patients or those with ascites
MR is preferable in alcoholic cirrhosis and for detection/distinction of hepatic nodules
– Include delayed phase MR or CT (5-10 minutes)
– Hepatobiliary MR contrast agents may aid in detection of HCC
Gadoxetate (Eovist, Primovist) is retained in normal liver, variably in cirrhotic liver, rarely in HCC
DIFFERENTIAL DIAGNOSIS
Treated Liver Metastases or Lymphoma
• Simulates nodules, fibrosis, volume loss of cirrhotic liver
• Breast carcinoma metastases to liver
May result in “pseudocirrhosis,” especially after treatment
Budd-Chiari Syndrome
• Liver damaged but usually no bridging fibrosis
Therefore, no true cirrhosis
Only gold members can continue reading. Log In or Register to continue









 to the edges of the caudate and right lobes, respectively. Note the bands of fibrosis
to the edges of the caudate and right lobes, respectively. Note the bands of fibrosis  and ascites.
and ascites.
 . Note the enlarged caudate lobe
. Note the enlarged caudate lobe  , which is as wide as the right lobe, although the caudate lobe is normally no more than 60% of the width of the right lobe.
, which is as wide as the right lobe, although the caudate lobe is normally no more than 60% of the width of the right lobe.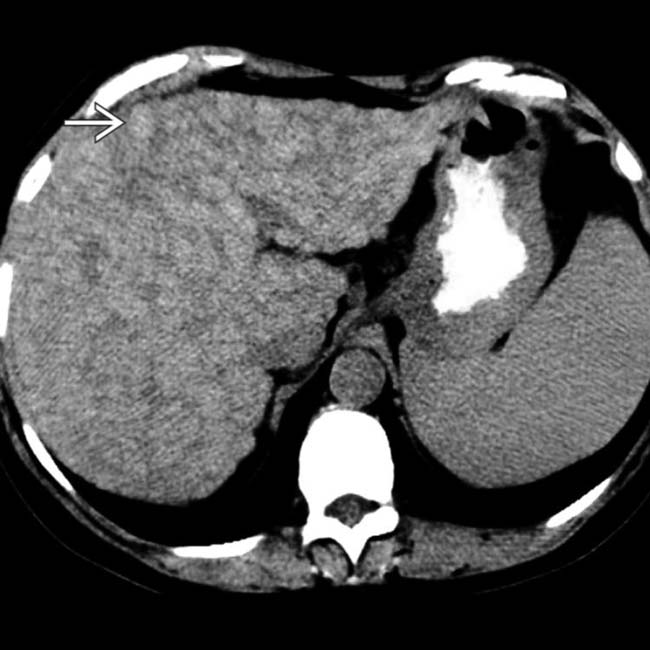
 , surrounded by lace-like fibrosis.
, surrounded by lace-like fibrosis.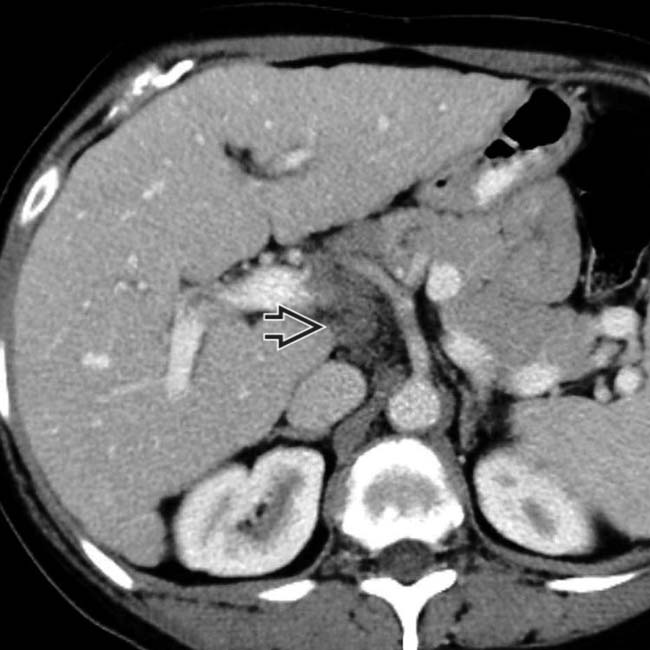
 , another typical feature of primary biliary cirrhosis, is also noted. Primary biliary cirrhosis is an autoimmune disease that typically affects women in their 5th or 6th decade.
, another typical feature of primary biliary cirrhosis, is also noted. Primary biliary cirrhosis is an autoimmune disease that typically affects women in their 5th or 6th decade.









 Arterioportal and portovenous shunts
Arterioportal and portovenous shunts















































