Simple congenital heart disease
Native disease
Isolated congenital aortic valve disease
Isolated congenital mitral valve disease (e.g., except parachute valve, cleft leaflet)
Small atrial septal defect
Isolated small ventricular septal defect (no associated lesions)
Mild pulmonary stenosis
Small patent ductus arteriosus
Repaired conditions
Previously ligated or occluded ductus arteriosus
Repaired secundum or sinus venosus atrial septal defect without residua
Repaired ventricular septal defect without residua
Congenital heart disease of moderate complexity
Aorto-left ventricular fistulas
Anomalous pulmonary venous drainage, partial or total
Atrioventricular septal defects (partial or complete)
Coarctation of the aorta
Ebstein’s anomaly
Infundibular right ventricular outflow obstruction of significance
Ostium primum atrial septal defect
Patent ductus arteriosus (not closed)
Pulmonary valve regurgitation (moderate to severe)
Pulmonary valve stenosis (moderate to severe)
Sinus of Valsalva fistula/aneurysm
Sinus venosus atrial septal defect
Sub- or supravalvular aortic stenosis (except hypertrophic obstructive cardiomyopathy)
Tetralogy of Fallot
Ventricular septal defect with:
Absent valve or valves
Aortic regurgitation
Coarctation of the aorta
Mitral disease
Right ventricular outflow tract obstruction
Straddling tricuspid/mitral valve
Subaortic stenosis
Congenital heart disease of great complexity
Conduits, valved or nonvalved
Cyanotic congenital heart disease (all forms)
Double outlet ventricle
Eisenmenger syndrome
Fontan procedure
Mitral atresia
Single ventricle (also called double inlet or outlet, common or primitive)
Pulmonary atresia (all forms)
Pulmonary vascular obstructive disease
Transposition of the great arteries
Tricuspid atresia
Truncus arteriosus/hemitruncus
Other abnormalities of atrioventricular or ventriculoarterial connection not included above (i.e., crisscross heart, isomerism, heterotaxy syndromes, ventricular inversion)
Incidence and Prevalence
Congenital heart defects are common [2, 11–13]. Their reported incidence varies among different studies depending on the type and setting of the study [13]. The number of patients with lesions of moderate to severe complexity seems to be relatively stable at around 6/1,000 live births with little variation between different countries and little changes over time [13]. Figure 1.1 depicts estimates of the incidence of various congenital heart defects at time of birth, derived from 44 studies of the incidence of congenital heart disease. Among all patients with CHD, ventricular septal defects are the most common defects by far, while among those with lesions of moderate or great complexity (bottom part of the Fig. 1.1), tetralogy of Fallot, complete transposition of the great arteries, and lesions with univentricular physiology have the highest incidence.
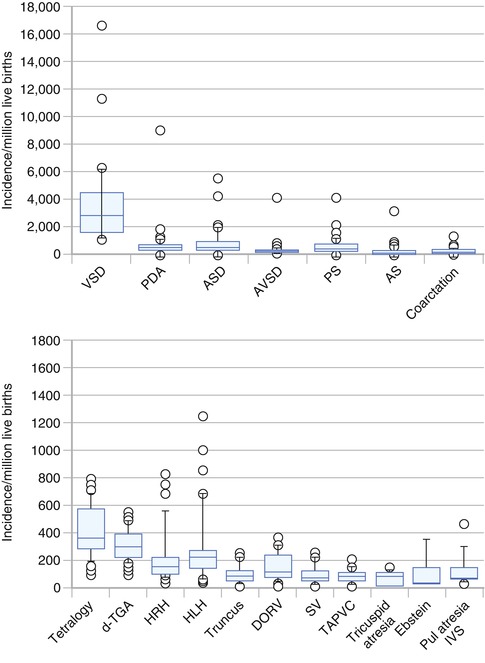
Fig. 1.1
Estimates on incidence of various types of congenital heart defects among live births. Modified box plots to show variability of the incidence per million live births of various forms of congenital heart disease. The rectangle shows the upper and lower quartiles, and the horizontal line in the middle is the median. The two short horizontal lines connected to the rectangle by thin vertical lines indicate the 90th and 10th percentiles, and data points outside these limits are shown individually. Each panel has a different vertical scale that on the top panel being ten times larger than that on the bottom panel. (Top) The four major left-to-right shunts (ventricular septal defect VSD, patent ductus arteriosus PDA, atrial septal defect ASD, atrioventricular septal defect AVSD) and the three major obstructive lesions (pulmonic stenosis PS, aortic stenosis AS, coarctation of the aorta coarctation). (Bottom) Tetralogy of Fallot (tetralogy); complete transposition of the great arteries (d-TGA); hypoplastic right heart HRH, which includes tricuspid atresia, Ebstein’s anomaly, and pulmonary atresia with an intact ventricular septum (pulmonary atresia IVS), hypoplastic left heart HLH, truncus arteriosus truncus, double outlet right ventricle DORV, single ventricle SV, total anomalous pulmonary venous connection TAPVC. The three components of the HRH syndrome do not add up to the total, because not all reports included all three (From Hoffman and Kaplan [13] with permission)
In the future, the increasing use of fetal echocardiography and subsequent therapeutic abortion for certain forms of complex CHD may affect their future incidence [14–16




Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
