Multiple colonic diverticula and colonic wall thickening
Inflammation of pericolonic fat (stranding)
Thickened base of sigmoid mesocolon
Engorged mesocolic blood vessels
“Microperforation”: Small bubbles of pericolonic gas
• More complicated diverticulitis
More extensive extraluminal collections of gas and fluid
Free intraperitoneal spread of gas or fluid
Fistulas to skin or hollow viscera
Infectious thrombophlebitis (pylephlebitis)
TOP DIFFERENTIAL DIAGNOSES
• Colon carcinoma
• Radiation colitis
• Ischemic colitis
• Pseudomembranous colitis
CLINICAL ISSUES
• Most common colonic disease in Western world
• Average age at onset is dropping
Related to obesity, metabolic syndrome, poor diet
• Percutaneous abscess drainage can obviate surgery or allow elective 1-step procedure in most cases
DIAGNOSTIC CHECKLIST
• Long segment colonic involvement, extensive inflammatory changes, and absence of nodes or metastases favor diverticulitis over colon cancer
• In some patients, it is difficult to distinguish diverticulitis from colon cancer; these should have follow-up endoscopy following resolution of acute symptoms
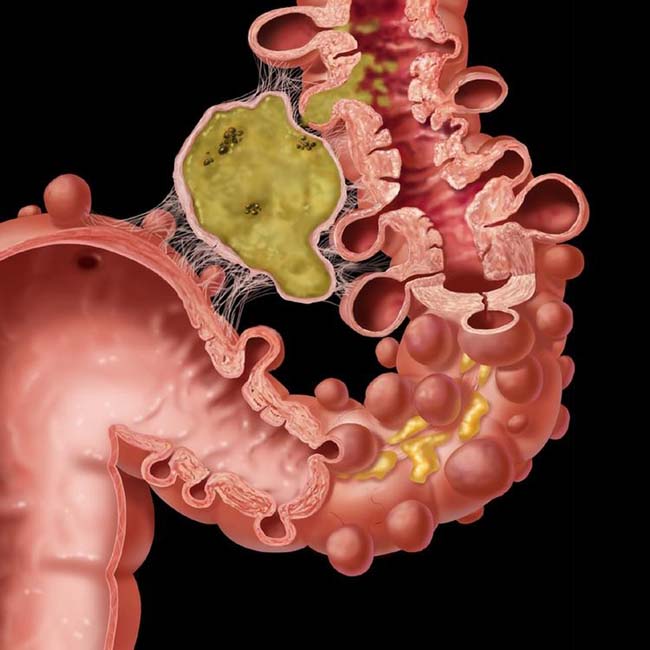
(Left) Graphic illustrates sigmoid diverticula, luminal narrowing, and wall thickening (circular muscle hypertrophy). There is a pericolic abscess due to the perforated diverticulum, but the rectum is spared.
(Right) Axial CECT shows uncomplicated sigmoid diverticulitis with irregular luminal narrowing and wall thickening, numerous gas-filled diverticula , and relatively mild infiltration of the pericolonic fat .
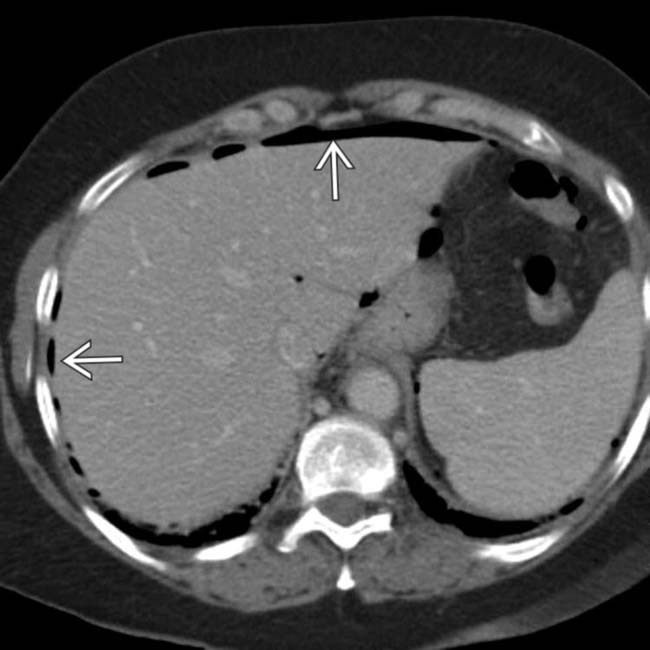
(Left) Axial CECT in a 60-year-old woman presenting with lower abdominal pain, fever, and tenderness demonstrates extensive free intraperitoneal gas .
(Right) Axial CECT in the same patient shows fluid that has loculated into abscesses . At surgery extensive sigmoid diverticulosis was discovered to be the source of the free air and abscesses. This amount of free intraperitoneal air is unusual as the omentum usually walls off the perforated diverticulum.
TERMINOLOGY
Definitions
• Intramural and pericolonic infectious/inflammatory process resulting from perforation of colonic diverticula.
IMAGING
General Features
• Best diagnostic clue
Diverticula, infiltrated pericolonic fat and engorged vessels, ± extraluminal gas and fluid
• Location
Most common in sigmoid colon (> 90% of cases)
Diverticula occur mainly where vasa recta vessels pierce muscularis propria, between mesenteric and antimesenteric taeniae
• Size
Diverticula usually 0.5-1.0 cm
• Morphology
• Colonic diverticula are pseudodiverticular
Saccular outpouchings of mucosa and submucosa, 5-10 mm in diameter
Fluoroscopic Findings
• Single contrast barium enema
Generally contraindicated in acute setting
Numerous diverticula are usually present as outpouchings from lumen
Colonic lumen is narrowed with serrated or “cog wheel” appearance
– Latter may represent spasm or result of circular muscle hypertrophy (not necessarily indicative of active inflammation)
CT Findings
• Diverticulosis
Multiple air-, contrast-, or stool-filled outpouchings (diverticula)
Colonic wall is often thickened
– May be due to circular muscle hypertrophy, not necessarily acute diverticulitis
• Diverticulitis
Simple or uncomplicated diverticulitis
– Multiple colonic diverticula and colonic wall thickening
Long segmental (> 10 cm) colonic involvement
– Inflammation of pericolonic fat (stranding)
Inflammation is usually localized by adherence of omentum
– Thickened base of sigmoid mesocolon; curvilinear line in left iliac fossa
– Engorged mesocolic blood vessels
– “Microperforation”: Small bubbles of pericolonic gas
More complicated diverticulitis
– More extensive extraluminal collections of gas &/or fluid (“macroperforation”)
May loculate as abscess with contrast-enhancing wall
– Free intraperitoneal spread of gas or fluid
Represents failure of omentum to wall off perforation
Generally requires surgical intervention for peritoneal soiling
– Fistulas to skin or hollow viscera
Enhancing tract with gas &/or enteric contrast material evident within bladder, vagina, etc.
– Infectious thrombophlebitis
Mesenteric vein becomes contaminated with colonic bacteria
May be evident as venous wall enhancement, luminal gas, or thrombosis
May carry gas and bacteria to portal vein and liver (potentially causing pyogenic hepatic abscess)
Ultrasonographic Findings
• Grayscale ultrasound
• Pericolic inflammation
Increased echogenicity ± ill-defined hypoechoic areas
• Pericolic abscess
Hypoechoic ± internal echoes
• Color and power Doppler
Hyperemia of pericolonic fat
Imaging Recommendations
• Best imaging tool
Multiplanar CECT
– Rectal contrast may be useful to demonstrate colonic fistulas
DIFFERENTIAL DIAGNOSIS
Colon Carcinoma
• Short segment involvement (< 10 cm), wall thickness > 2 cm, mesenteric lymphadenopathy, metastases










 , and relatively mild infiltration of the pericolonic fat
, and relatively mild infiltration of the pericolonic fat  .
.
 .
.
 . At surgery extensive sigmoid diverticulosis
. At surgery extensive sigmoid diverticulosis  was discovered to be the source of the free air and abscesses. This amount of free intraperitoneal air is unusual as the omentum usually walls off the perforated diverticulum.
was discovered to be the source of the free air and abscesses. This amount of free intraperitoneal air is unusual as the omentum usually walls off the perforated diverticulum.









 Simple or uncomplicated diverticulitis
Simple or uncomplicated diverticulitis













 Acute radiation colitis/proctitis
Acute radiation colitis/proctitis





