Pseudodiverticula balloon-out between areas of fibrosis and spasm
“Cloverleaf” deformity of bulb due to pseudodiverticula
• CT with IV and oral contrast medium for diagnosis of perforation
Wall thickening, luminal narrowing of duodenum
Extraluminal intra- or retroperitoneal gas ± enteric contrast medium
TOP DIFFERENTIAL DIAGNOSES
• Duodenal inflammation
• Duodenal stricture
• Duodenal carcinoma
CLINICAL ISSUES
• 2-3x more frequent than gastric ulcers
• Burning, gnawing, or aching pain at epigastrium 2-4 hours after meals, relieved by antacids/food
• Pain episodes occurring in clusters of days to weeks followed by longer pain-free intervals
DIAGNOSTIC CHECKLIST
• Barium upper GI series and CT are complementary in diagnosis of ulcers and complications
• Eradication of Helicobacter pylori is 1st step of treatment
Proton-pump inhibitors are also effective
• Effective medical treatment has made surgical treatment much less common
(Left) Graphic illustrates a duodenal ulcer with a deformed bulb due to converging folds and spasm.
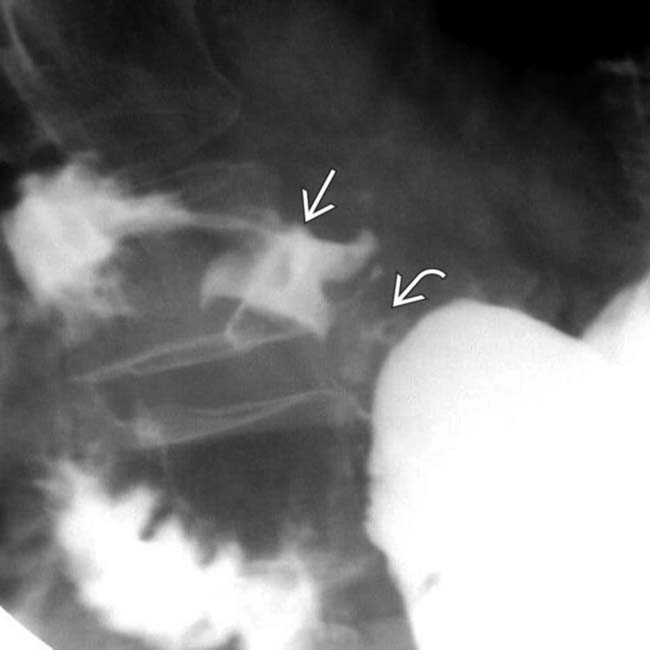
(Right) Film from an upper GI series shows a “cloverleaf” deformation of the duodenal bulb, with the ulcer at the center of the cloverleaf. The other lobes of the cloverleaf are the duodenal bulb fornices or recesses. The pylorus is marked for orientation.
(Left) Axial CECT in a 42-year-old man presenting with acute severe abdominal pain and guarding shows extensive free intraperitoneal gas from a perforated duodenal ulcer.
(Right) Axial CECT in the same patient demonstrates a thickened gastric wall , probably due to gastritis. Ventral to the duodenal bulb and antrum are small collections of extraluminal gas and oral contrast medium that confirm an ulcer as the source of perforation.
TERMINOLOGY
Synonyms
• Peptic ulcer disease
Definitions
• Mucosal erosion of duodenum
IMAGING
General Features
• Best diagnostic clue
Sharply marginated barium collection with folds radiating to edge of ulcer crater on upper GI series
• Location
95% of ulcers are in duodenal bulb, 5% postbulbar
– Bulbar ulcers: Apex, central portion, or base of bulb
– Postbulbar ulcers: Medial wall of proximal descending duodenum above papilla of Vater






 at the center of the cloverleaf. The other lobes of the cloverleaf are the duodenal bulb fornices or recesses. The pylorus
at the center of the cloverleaf. The other lobes of the cloverleaf are the duodenal bulb fornices or recesses. The pylorus  is marked for orientation.
is marked for orientation.
 from a perforated duodenal ulcer.
from a perforated duodenal ulcer.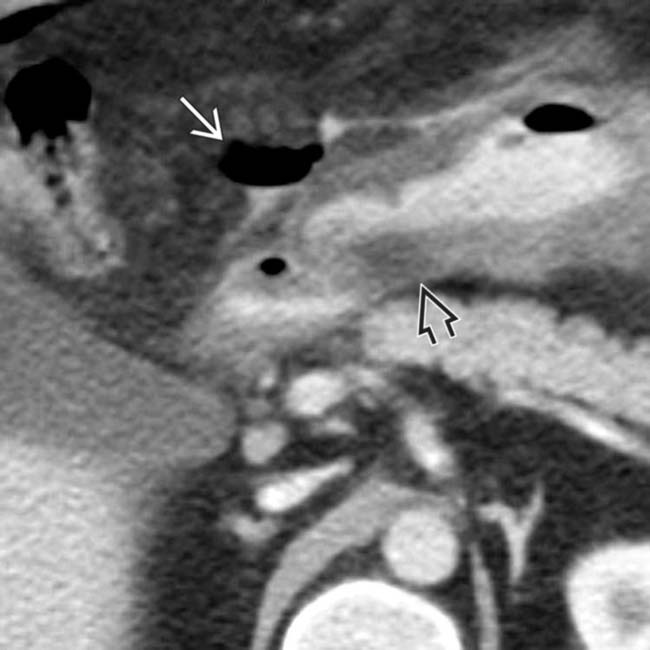
 , probably due to gastritis. Ventral to the duodenal bulb and antrum are small collections of extraluminal gas and oral contrast medium
, probably due to gastritis. Ventral to the duodenal bulb and antrum are small collections of extraluminal gas and oral contrast medium  that confirm an ulcer as the source of perforation.
that confirm an ulcer as the source of perforation.














 1 or more strictures in 2nd or 3rd portions of duodenum → marked obstruction, proximal dilatation (megaduodenum)
1 or more strictures in 2nd or 3rd portions of duodenum → marked obstruction, proximal dilatation (megaduodenum)











