• Complication rates vary substantially according to experience and skill of surgical team
Open surgical procedures tend to result in higher perioperative morbidity and mortality
High (cervical) anastomoses result in slightly higher incidence of injury to laryngeal nerve
(Left) Graphic illustrates the 1st step in an esophagectomy with gastric interposition. The stomach is divided along its long axis, creating a gastric tube or conduit 5 or 6 cm in diameter, which is pulled up into the chest. This can be done through a right (Ivor Lewis) or left thoracotomy or even through laparoscopic ports. A pyloroplasty is done to facilitate gastric emptying.
(Right) Graphic shows the gastric conduit anastomosed to the mid esophagus and the pyloroplasty .
(Left) Graphic shows the gastric conduit anastomosed to the cervical esophagus. Note the position of the gastric staple line along the right side of the conduit.
(Right) Axial CT shows a mildly dilated, gas-filled gastric conduit in the paravertebral location. Note the position of the gastric staple line . The conduit is not filled with retained fluid, and there is no evidence of lung injury from reflux.
TERMINOLOGY
Definitions
• Surgical resection of portion of esophagus and replacement by conduit formed by another portion of alimentary tube
IMAGING
Surgical Procedures
• Usual indication for surgery
Curative or palliative resection of esophageal carcinoma
Resection of Barrett esophagus with severe dysplasia
• Many surgical options for surgical excision of portion of esophagus
• Transthoracic esophagectomy
Usually performed through right intercostal approach (Ivor Lewis procedure)
– Generally begins with laparotomy for mobilization of stomach, which is then used to create gastric tube/conduit that will replace resected esophagus
Either entire stomach or tubularized portion (divided along long axis) is used
Stomach is ideal conduit, as it has reliable blood supply and can reach high into thorax or neck for anastomosis
– As part of laparotomy, upper abdominal lymph nodes (celiac, gastrohepatic) are resected
– Pyloroplasty or pyloromyotomy is performed to facilitate gastric emptying and to minimize gastroesophageal reflux
– At thoracotomy, esophagus and thoracic duct are dissected from vertebral column
– Esophagus and regional lymph nodes (mediastinum and neck) are resected en bloc
– Esophagogastric anastomosis is created in thorax, above level of tracheal carina
Some surgeons make anastomosis in lower neck
– Gastric conduit is usually placed in pre- or paravertebral space of posterior mediastinum
Less commonly in retrosternal, intrapleural, or subcutaneous position
– Colon and jejunum are used much less commonly to bypass or replace resected (or obstructed) esophagus
Usually after failed gastric interposition
Many variations exist
– e.g., left thoracotomy approach, transhiatal open approach (without thoracotomy), minimally invasive procedures (performed through ports in thorax and abdomen without open incision into either)
– Surgical approach may be affected by patient condition (site and depth of tumor, mediastinal scarring from prior surgery, etc.)
– Experience and preference of surgeon play larger role in surgical approach
Complication rates
– No proof of significantly different morbidity or mortality among various surgical approaches
Complication rates vary substantially according to experience and skill of surgical team
– Open surgical procedures tend to result in slightly higher perioperative morbidity and mortality
– High (cervical) anastomoses result in slightly higher incidence of injury to laryngeal nerve
Contraindications to esophagectomy (relative or absolute)






 Essentially all patients have some degree of dysphagia, early satiety, and reflux following esophagectomy
Essentially all patients have some degree of dysphagia, early satiety, and reflux following esophagectomy






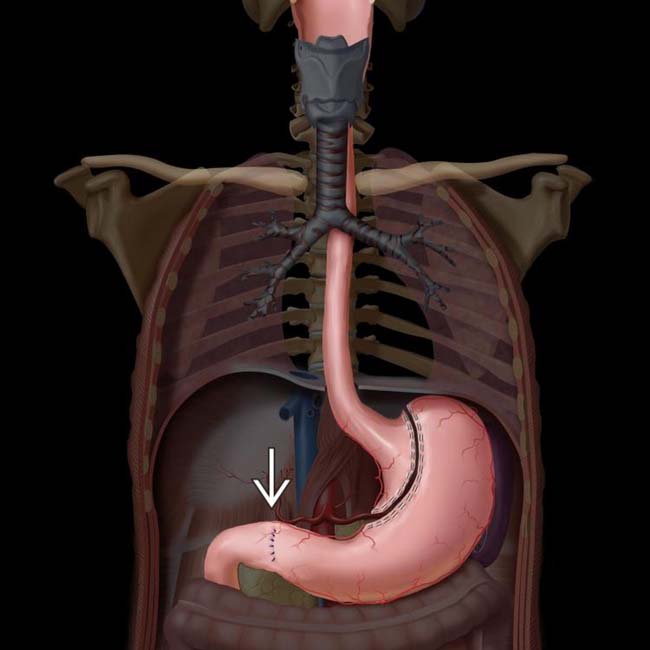
 is done to facilitate gastric emptying.
is done to facilitate gastric emptying.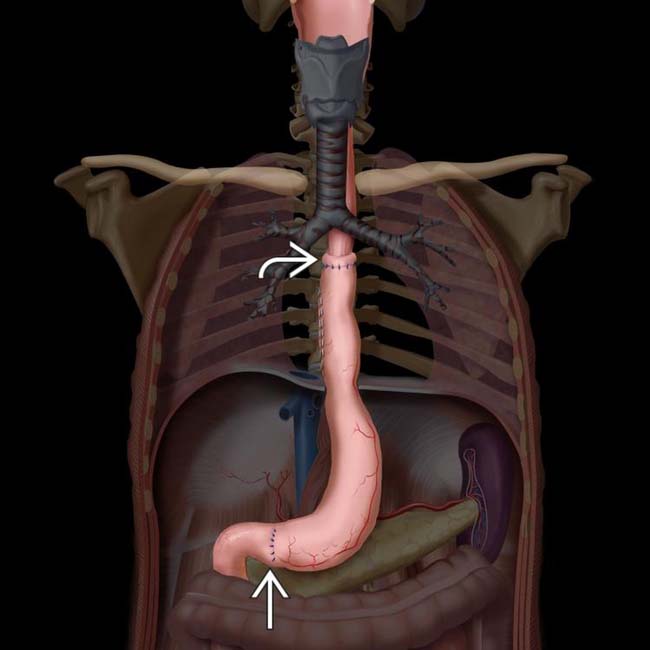
 and the pyloroplasty
and the pyloroplasty  .
.
 anastomosed to the cervical esophagus. Note the position of the gastric staple line
anastomosed to the cervical esophagus. Note the position of the gastric staple line  along the right side of the conduit.
along the right side of the conduit.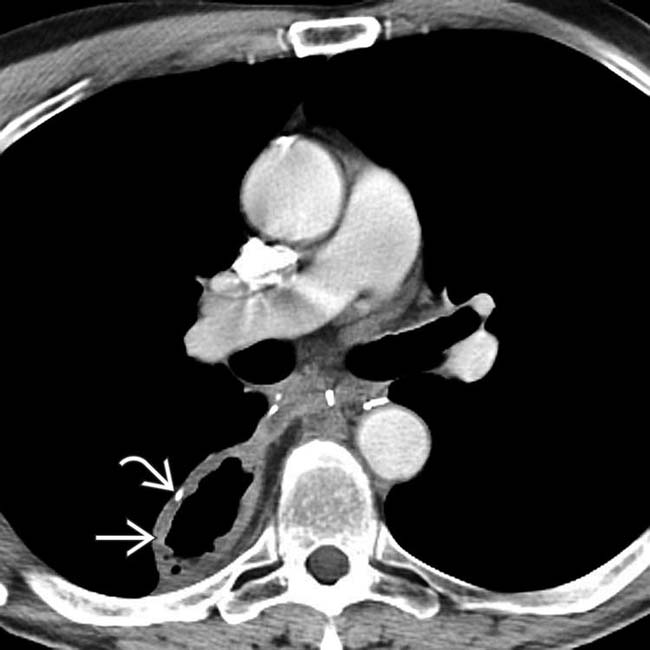
 in the paravertebral location. Note the position of the gastric staple line
in the paravertebral location. Note the position of the gastric staple line  . The conduit is not filled with retained fluid, and there is no evidence of lung injury from reflux.
. The conduit is not filled with retained fluid, and there is no evidence of lung injury from reflux.

 Usually performed through right intercostal approach (Ivor Lewis procedure)
Usually performed through right intercostal approach (Ivor Lewis procedure) Many variations exist
Many variations exist Complication rates
Complication rates






 Injury to recurrent laryngeal or vagus nerve (5-10%)
Injury to recurrent laryngeal or vagus nerve (5-10%) Injury to tracheobronchial tree
Injury to tracheobronchial tree







