• Also known as fibrolamellar hepatocellular carcinoma (HCC)
Distinct clinical, histopathologic, and imaging features differentiate it from conventional HCC
IMAGING
• Heterogeneously enhancing, large, lobulated mass with hypointense central scar and radial septa
Calcification and necrosis are common (> 50%)
Nodal metastases (> 50%)
Vary from 5-20 cm (mean: 13 cm)
“Satellite” nodules are often present
• Slow-growing tumor that usually arises in normal (noncirrhotic) liver
• Better prognosis than conventional HCC but still locally invasive and frequently metastatic
TOP DIFFERENTIAL DIAGNOSES
• Focal nodular hyperplasia (FNH)
• Conventional HCC
• Hepatic cavernous hemangioma
• Peripheral cholangiocarcinoma
DIAGNOSTIC CHECKLIST
• FLC simulates FNH due to presence of central scar in both tumors
FLC: Bigger, more heterogeneous mass frequently with calcified central/eccentric scar and features of malignancy (vessel &/or biliary obstruction, nodal invasion, and lung metastases)
Scar on T2WI: Hypointense in FLC, hyperintense in FNH
• Large, heterogeneous, hypervascular tumor in young adult
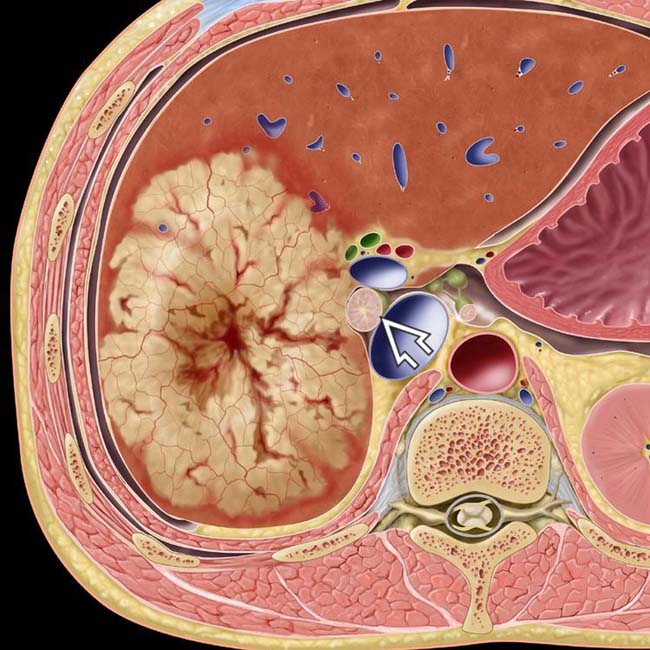
(Left) Axial graphic shows a large, heterogeneous, hypervascular mass with a central scar and porta hepatis lymphadenopathy .
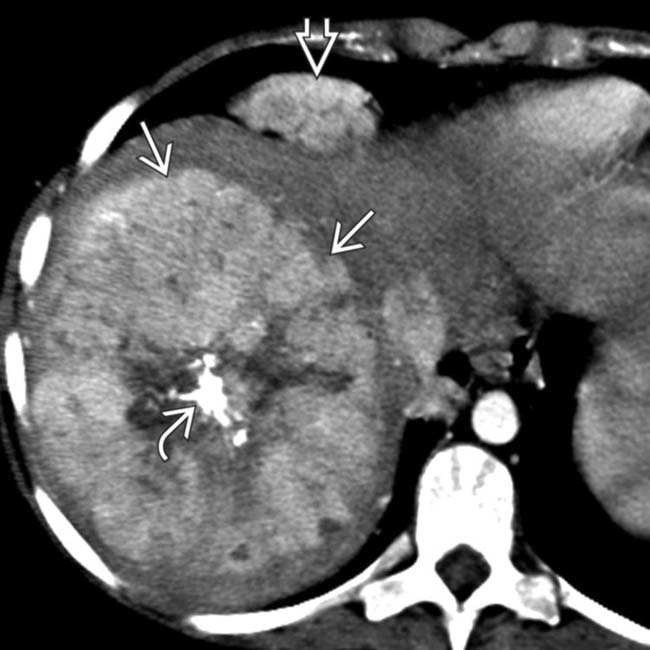
(Right) Axial CECT in a 15-year-old boy shows a large, heterogeneous, hypervascular mass with a large, calcified central scar and cardiophrenic lymphadenopathy . In a young person, these findings are essentially diagnostic of fibrolamellar carcinoma (FLC)
(Left) Axial CECT of a 22-year-old man with abdominal discomfort and a palpable mass shows a large, heterogeneous, lobulated mass with a large central scar containing foci of calcification . Scar calcification is very rare in focal nodular hyperplasia (FNH), by comparison.
(Right) Gross pathology of the same patient’s resected tumor shows a well-demarcated, lobulated, heterogeneous tumor with bile staining and central or eccentric fibrous scars , typical features of FLC.
TERMINOLOGY
Abbreviations
• Fibrolamellar carcinoma (FLC) of liver
Synonyms
• Fibrolamellar hepatocellular carcinoma
Definitions
• Uncommon malignant hepatocellular tumor
Distinct clinical, histopathologic, and imaging features differentiate it from conventional hepatocellular carcinoma (HCC)
IMAGING
General Features
• Best diagnostic clue
Heterogeneously enhancing, large, lobulated mass with hypointense central scar and radial septa
• Location
Intrahepatic (80%)
Pedunculated (20%)
• Size
5-20 cm (mean: 13 cm)
• Key concepts
Slow-growing tumor that usually arises in normal (noncirrhotic) liver
– May occur with underlying cirrhosis (< 5% of cases)







 .
.
 with a large, calcified central scar
with a large, calcified central scar  and cardiophrenic lymphadenopathy
and cardiophrenic lymphadenopathy  . In a young person, these findings are essentially diagnostic of fibrolamellar carcinoma (FLC)
. In a young person, these findings are essentially diagnostic of fibrolamellar carcinoma (FLC)
 with a large central scar containing foci of calcification
with a large central scar containing foci of calcification  . Scar calcification is very rare in focal nodular hyperplasia (FNH), by comparison.
. Scar calcification is very rare in focal nodular hyperplasia (FNH), by comparison.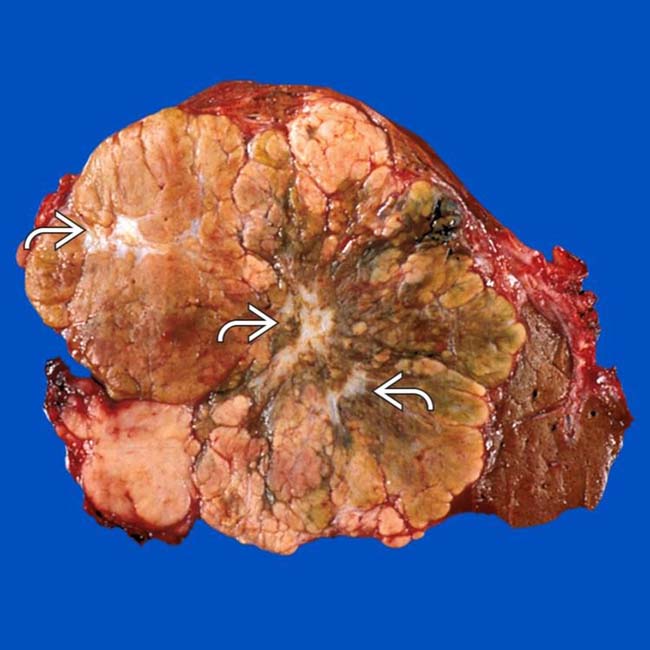
 , typical features of FLC.
, typical features of FLC.


























 Mass
Mass





