Central scar: Hyperdense or hyperintense (due to fibrous tissue)
• Gadoxetate-enhanced MR
Most specific test to diagnose FNH
Prolonged enhancement of entire FNH (except scar) on delayed scan
TOP DIFFERENTIAL DIAGNOSES
• Hepatic adenoma
Rarely retains gadoxetate on delayed phase MR
• Fibrolamellar hepatocellular carcinoma
Usually large (> 12 cm) heterogeneous mass
Has “aggressive” features such as metastases
• Hepatic cavernous hemangioma
Enhanced portions isodense to vessels
• Hypervascular metastasis
Usually multiple with known primary tumor
DIAGNOSTIC CHECKLIST
• Imaging is more reliable than histology in establishing diagnosis of FNH
• Diagnosis can be made by CT alone in most cases
MR with gadoxetate enhancement is most specific test
(Left) Graphic shows a homogeneous, vascular, nonencapsulated mass with a central scar and thin radiating septa dividing the mass into hyperplastic nodules. Note the cluster of small arteries near the central scar.
(Right) Axial arterial phase CECT shows bright, homogeneous enhancement of a mass with a central scar in an asymptomatic young woman who had a mass found on ultrasound. The CT findings in this case are diagnostic of FNH and require no further evaluation.
(Left) This liver wedge resection shows a well-circumscribed nodular lesion with a central stellate scar , typical of FNH. (Courtesy M. Yeh, MD, PhD.)
(Right) The central scar as well as the fibrous septa may contain thick-walled vessels . (Courtesy M. Yeh, MD, PhD.)
TERMINOLOGY
Abbreviations
• Focal nodular hyperplasia (FNH)
Definitions
• Benign tumor of liver caused by hyperplastic response to localized vascular abnormality
IMAGING
General Features
• Best diagnostic clue
Bright, homogeneously enhancing mass on arterial phase CT or MR with delayed enhancement of central scar
– Hyperintense enhancement on hepatobiliary phase of gadoxetate-enhanced MR
• Location
Usually subcapsular and rarely pedunculated
• Size
Majority are < 5 cm unless symptomatic
• Morphology
Spherical nonencapsulated mass
• Key concepts
2nd most common benign tumor of liver
Benign congenital hamartomatous malformation
Accounts for 8% of primary hepatic tumors in autopsy series
Usually solitary lesion (80%); multiple (20%)
Multiple FNHs are associated with multiorgan vascular malformations and certain brain neoplasms
CT Findings
• NECT
Isodense or hypodense to normal liver
• CECT
Hepatic arterial phase scan
– Transient, intense, homogeneous hyperdensity
Portal venous phase scan
– Hypodense or isodense to normal liver
– Large draining veins → hepatic veins
Delayed scans
– Mass: ∼ isodense to normal liver
– Central scar: Hyperdense (due to fibrous tissue)
– Scar visible in 2/3 of large and 1/3 of small FNHs
“Large” > 3 cm
MR Findings
• T1WI
Mass: Isointense to slightly hypointense
Central scar: Hypointense
• T2WI
Mass: Slightly hyperintense to isointense
Central scar: Hyperintense
• T1WI C+
Arterial phase: Hyperintense (homogeneous)
Portal venous: Isointense to liver
Delayed phase
– Mass: Isointense
– Scar: Hyperintense
• Specific hepatobiliary MR contrast agents
Gadoxetate (Eovist or Primovist)
– Bright, homogeneous enhancement of FNH on arterial phase
– Prolonged enhancement of entire FNH on hepatobiliary phase (delayed, ∼ 20 minutes)
Intensity of FNH > liver
Most specific test to distinguish from all other hepatic masses
Due to functioning hepatocytes, malformed bile ductules
Ultrasonographic Findings
• Grayscale ultrasound
Mass: Mostly homogeneous and isoechoic to liver
– Occasionally hypoechoic or hyperechoic
Central scar: Hypoechoic
• Color Doppler
Spoke-wheel pattern
– Large central feeding artery with multiple small vessels radiating peripherally
Large draining veins at tumor margins
High-velocity Doppler signals
– Due to increased blood flow or arteriovenous shunts
Angiographic Findings
• Conventional
Arterial phase
– Tumor: Hypervascular
– Scar: Hypovascular
– Enlargement of main feeding artery with centrifugal blood supply
– Same spoke-wheel pattern as on color Doppler
Only gold members can continue reading. Log In or Register to continue










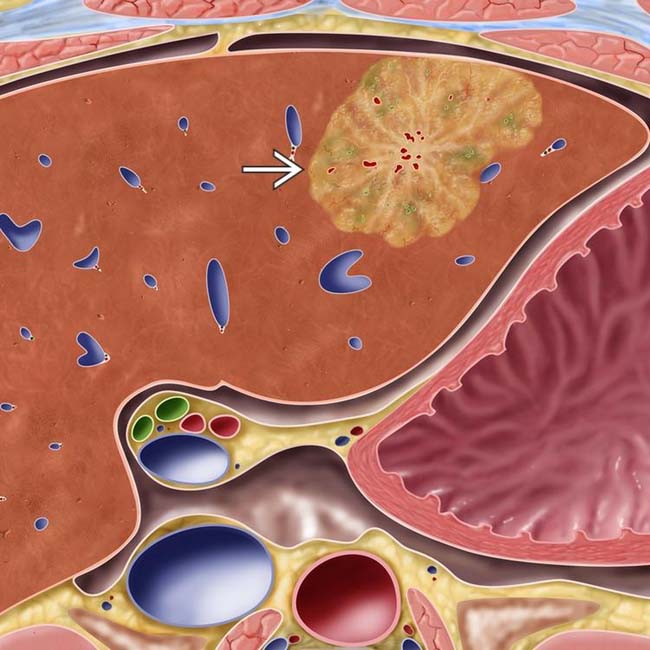
 with a central scar and thin radiating septa dividing the mass into hyperplastic nodules. Note the cluster of small arteries near the central scar.
with a central scar and thin radiating septa dividing the mass into hyperplastic nodules. Note the cluster of small arteries near the central scar.
 with a central scar
with a central scar  in an asymptomatic young woman who had a mass found on ultrasound. The CT findings in this case are diagnostic of FNH and require no further evaluation.
in an asymptomatic young woman who had a mass found on ultrasound. The CT findings in this case are diagnostic of FNH and require no further evaluation.
 , typical of FNH. (Courtesy M. Yeh, MD, PhD.)
, typical of FNH. (Courtesy M. Yeh, MD, PhD.)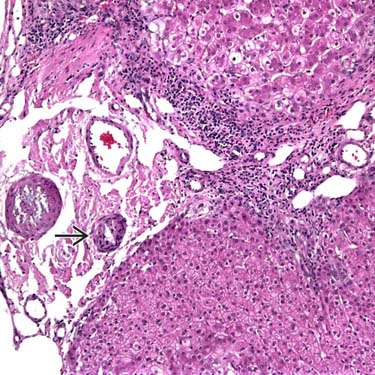
 . (Courtesy M. Yeh, MD, PhD.)
. (Courtesy M. Yeh, MD, PhD.)





























 Arterial phase
Arterial phase





