Joan Williams, George M. Bridgeforth, and Charles Carroll IV
A 2-year-old male infant fell from his high chair. He acts as if his left arm, which is swollen and tender, hurts.

CLINICAL POINTS
- Causes include sports and trauma.
- A fracture of the proximal (or middle ulna) is associated with a dislocation of the radial head.
- Forearm fractures are often open fractures.
During physical examination for patients with all types of forearm injuries, the physician should
- palpate the wrist, elbow, and shoulder to assess for associated injuries, because often these fractures are a result of high-speed injury.
- conduct a thorough neurovascular examination. It is important to pay special attention to the radial, ulnar, and median nerves, including evaluation of the anterior interosseous and posterior interosseous nerve branches. With neurovascular damage, the patient will manifest diminished or absent pulses. Moreover, the extremity will be cold. Motor strength will be severely affected and will be absent or pain limited. In addition, accompanying sensory abnormalities which are characterized by decreased pinprick and light touch are common findings as well. Neurovascular impairment may occur as the result of a compartment syndrome or from direct trauma to the neurovascular structures. The damaged extremity usually demonstrates pallor in fair-skinned individuals. However, this may not be present in dark-skinned patients. It is essential to document the neurovascular examination carefully.
- evaluate for compartment syndrome. The most sensitive clinical test for this is pain with passive extension of the fingers. There is marked swelling of the arm. The increased pressure inside the forearm is diminishing the blood flow to the extremities. The presence of a radial pulse does not rule out compartment syndrome; capillary blood flow ceases at a pressure lower than arterial blood flow.
- Check for open wounds on the forearm, because these injuries are frequently open fractures.
CLINICAL PRESENTATION
Nearly 50% Of Fractures Affect The Arm. Fractures Of The Forearm Are Most Often Due To Direct Blows, Although They May Also Occur With Falls Onto An Outstretched Hand. It Is Important To Recognize That The Forearm, Which Consists Of The Radius And Ulna, Acts As A Ring And That Dissipation Of Energy Results In Fractures Or Dislocations Of Both Bones In Most Cases. These Fractures May Be Classified According To Their Occurrence On The Proximal, Middle, Or Distal Shafts Of The Radius And Ulna. With Forearm Fractures, Associated Injuries May Occur In The Elbow And Wrist.
MONTEGGIA FRACTURE
A Monteggia fracture is a fracture of the proximal ulna with an associated radial head dislocation (Fig. 36.1). The majority (60%) of these injuries involve anterior dislocation of the radial head. Anterior and lateral dislocations are seen primarily in children. Posterior dislocations are seen primarily in adults.
GALEAZZI FRACTURE
A Galeazzi fracture is a fracture of the radial diaphysis at the junction of the middle and distal thirds (Figs. 36.2, 36.3). Also known as a reverse Monteggia fracture, it is associated with disruption of the distal radioulnar joint (DRUJ).
NIGHTSTICK FRACTURE
A nightstick fracture is an isolated fracture of the ulnar shaft, most often due to direct trauma to the ulna (Fig. 36.4). The forearm is usually held in protection across the face (Fig. 36.5).
Radiographic Evaluation
Radiographs to order include anteroposterior (AP) and lateral films of the forearm. If necessary, the examiner may obtain oblique views of the forearm for further fracture definition. Elbow and wrist films of the injured extremity are important to obtain, because forearm radiographs are not adequate for ruling out associated wrist and elbow injuries.
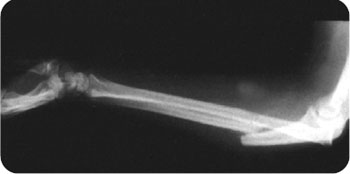
FIGURE 36.1 Type II Bado fracture with a posterolateral dislocation of the radial head in a 26-year-old woman. (From Bucholz RW, Heckman JD. Rockwood and Green’s Fractures in Adults. 5th ed. Philadelphia, PA: Lippincott, Williams & Wilkins; 2001.)
MONTEGGIA FRACTURE
In both the AP and lateral views, the radial head should be in line with the capitellum. A vertical line drawn along the anterior border of the humerus on the lateral view should intersect a horizontal line that bisects the long axis of the radius at the middle third of the capitellum. The absence of these relationships indicates a dislocation of the radial head (Fig. 36.6).

FIGURE 36.2 Severely displaced Galeazzi fracture–dislocation in lateral projection. The distal radioulnar dislocation (open arrow) is secondary to the marked shortening of the radius caused by the severe ulnar displacement and dorsal angulation of the distal radial fragment. (From Harris JH Jr, Harris WH. The Radiology of Emergency Medicine. 3rd ed. Philadelphia, PA: Lippincott-Raven; 2000:390, with permission.)
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


