• CT for severe abdominal or chest pain, suspected visceral injury, or abscess
DIAGNOSTIC CHECKLIST
• Postoperative fluoroscopic evaluation should be used liberally or even routinely
• CT for suspected leak or bleeding
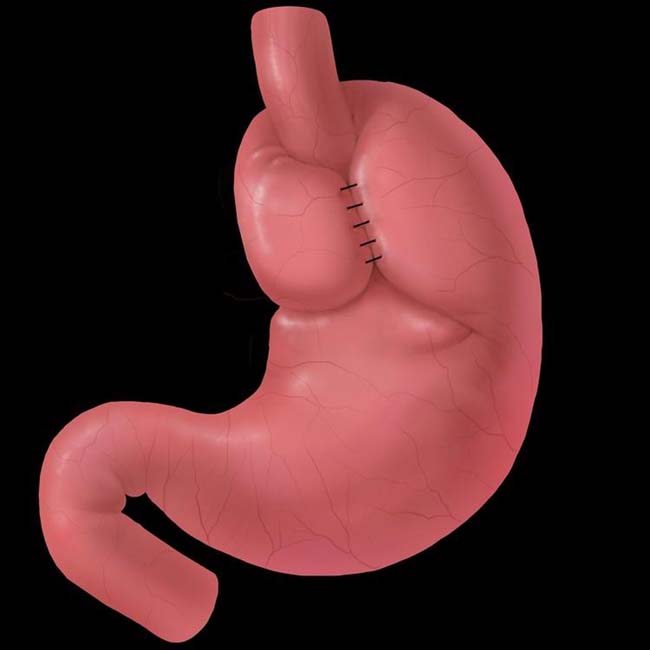
(Left) Graphic shows a Nissen fundoplication (FDP) with the gastric fundus wrapped completely (360°) around the gastroesophageal junction.
(Right) Upright spot film from an esophagram performed soon after a Nissen FDP shows an intact wrap in its expected subdiaphragmatic location as a filling defect within the air-filled fundus. The distal 3 cm of the esophageal lumen is compressed as it passes through the wrap.
(Left) A supine film from the same study shows the intact wrap as a filling defect with the barium pool in the fundus.
(Right) Axial NECT shows an intact FDP as a soft tissue density mass within the gastric fundus. The metallic staple line is evident within the wrap. The mass effect of the wrap tends to decrease with time following surgery.
TERMINOLOGY
Abbreviations
• Fundoplication (FDP)
Definitions
• Complications of antireflux surgery for management of gastroesophageal reflux disease (GERD)
• Nissen FDP: Complete (360°) FDP
Approach: Laparoscopic or open FDP
Gastric fundus wrapped 360° around intraabdominal esophagus to create antireflux valve
Concomitant hiatial hernia is reduced; diaphragmatic esophageal hiatus sutured
• Toupet FDP: Partial (270°) FDP
Posterior hemivalve created
• Belsey Mark IV repair: Open surgical; 240° FDP wrap around left lateral aspect of distal esophagus
Fundus sutured to intraabdominal esophagus; acute esophagogastric junction angle (angle of His)
Can also be performed via minimally invasive techniques
IMAGING
General Features
• “Wrap” complications
Slipped or misplaced FDP
FDP disruption or breakdown
FDP herniation with intrathoracic migration
Too tight, too loose, or too long FDP
Herniation of stomach through diaphragmatic hiatus
• “Non-wrap” complications
Injury to intraabdominal, intrathoracic organs
Leaks: Intraabdominal, intrathoracic
Mediastinal collection of gas and fluid (blood, transudate, or pus)
Fistulas; gastropericardial, gastrobronchial, etc.
Pneumothorax, pneumonia, pancreatitis, incisional hernia, mesenteric and portal venous thrombosis
• Late complications
Recurrent paraesophageal herniation
Distal esophageal stricture
Radiographic Findings
• Fluoroscopy
• Preoperative evaluation is critical to identify
Presence, type and size of hiatal hernia (HH)
Irreducible HH or “short esophagus”
– Stomach is pulled taut into chest; does not return to abdomen on upright positioning
– May require Collis gastroplasty (effectively lengthening esophagus by creating a gastric tube)
– Wrap goes around “neoesophagus” in abdomen = Nissen-Collis FDP
Also evaluate for reflux and esophageal motility
– FDP is relatively contraindicated in patients with severe dysmotility
• Normal postoperative appearance
Nissen FDP wrap: Well-defined mass in gastric fundus; smooth contour and surface
– Distal esophagus tapers smoothly through center of symmetric compression by wrap
– Tapered segment 2-3 cm long
– Pseudotumoral defect within gastric fundus = wrap
Defect more pronounced for complete wrap of Nissen than partial wrap of Toupet, Belsey
Best detected on upright film (wrap outlined by air in fundus), or supine (wrap as filling defect in barium pool)
Toupet (partial, posterior) FDP
– Barium may fill portions of wrap
Don’t mistake for leak or dehiscence
Distal esophagus should still be “squeezed”
Nissen-Collis procedure
– Gastroesophageal (GE) junction (at B ring) will be above diaphragm
– Intact wrap around proximal stomach (neoesophagus) will be below diaphragm
Look for gastric folds within neoesophagus
Belsey Mark IV repair
– Wrap produces smaller defect than Nissen FDP
– 2 distinct angles form as esophagus passes FDP
– Shallow upper angle; where esophagus, fundus, and diaphragm suture together
– Steep lower angle; where stomach pulled upward
• “Wrap” complications
Tight FDP wrap
– Fixed narrowing of distal esophagus with delayed emptying
– May also see gas distention of stomach (gas bloat syndrome)
– May also be caused by excessive closure of esophageal hiatus of diaphragm
Complete disruption (dehiscence) of FDP sutures
– Findings may resemble those of normal patient who has had no surgery
– Recurrent hiatal hernia and gastroesophageal reflux
– Gastric outpouching above diaphragm
– Expected mass of FDP wrap and narrowing of distal esophagus are not seen
Partial disruption of FDP sutures
– Partially intact wrap; does not squeeze distal esophagus
Only gold members can continue reading. Log In or Register to continue








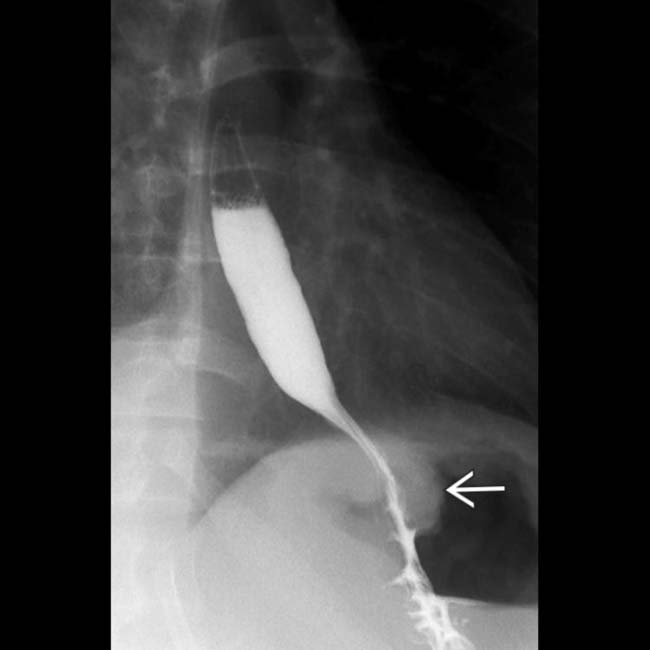
 in its expected subdiaphragmatic location as a filling defect within the air-filled fundus. The distal 3 cm of the esophageal lumen is compressed as it passes through the wrap.
in its expected subdiaphragmatic location as a filling defect within the air-filled fundus. The distal 3 cm of the esophageal lumen is compressed as it passes through the wrap.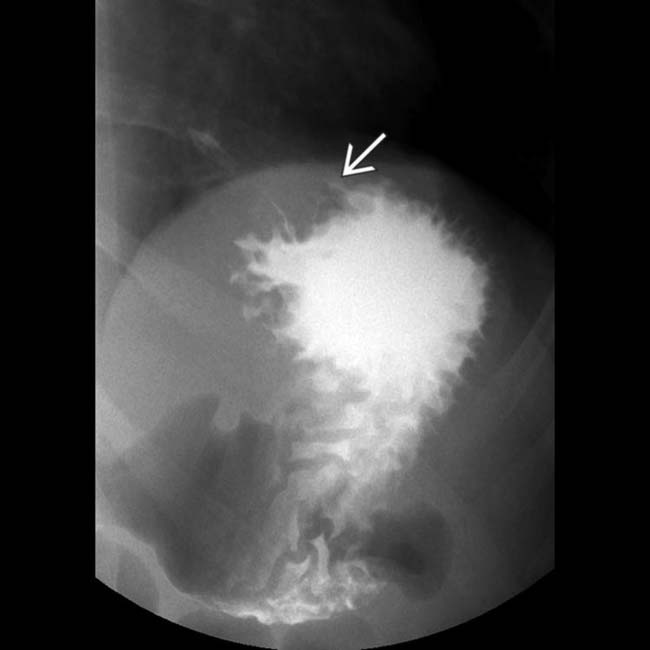
 as a filling defect with the barium pool in the fundus.
as a filling defect with the barium pool in the fundus.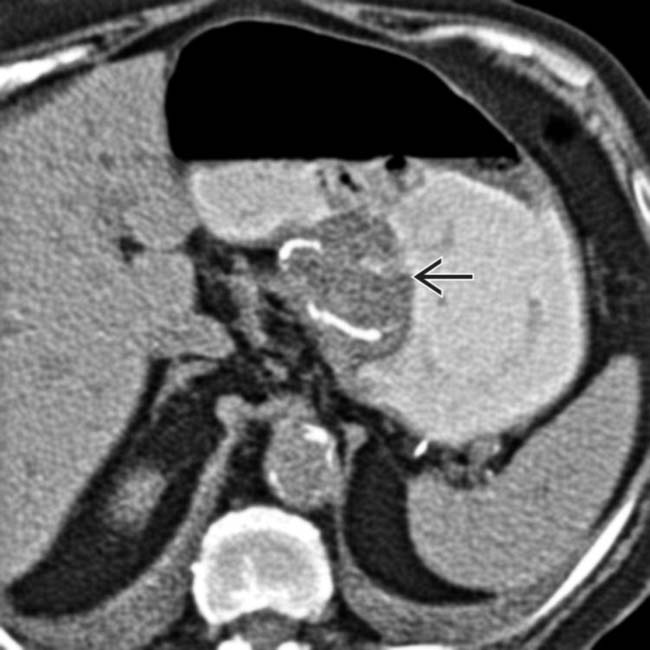
 within the gastric fundus. The metallic staple line is evident within the wrap. The mass effect of the wrap tends to decrease with time following surgery.
within the gastric fundus. The metallic staple line is evident within the wrap. The mass effect of the wrap tends to decrease with time following surgery.





























 Partial disruption of FDP sutures
Partial disruption of FDP sutures







