Choledocholithiasis: Stones within common bile duct (CBD)
• Sludge: Suspension of particulate material/bile in gallbladder (GB)
IMAGING
• Gallstones
Ultrasound: Brightly echogenic nodule with marked posterior acoustic shadowing
– Mobile with “twinkling” on color Doppler images
– Wall-echo-shadow sign when GB is filled with stones
Anterior wall of GB is demarcated by echogenic line (“wall”), deep to which is a layer of bile demarcated by hypoechoic line (“echo”), followed by posterior acoustic shadowing from most superficial stones (“echo”)
MR: Stones most conspicuous on T2WI and MRCP
– Usually low signal (signal void) on T1WI and T2WI
– MRCP better than CT/US for CBD stones
CT: Overall sensitivity of CT for stones is roughly 80%
– 20% of stones are not identified on CT, often “pure” cholesterol stones, which are isodense to bile
Radiographs: Only 10-20% of cholesterol stones are visible on radiographs
• Sludge
Layering, mobile material in dependent portion of GB
Variable echogenicity with no acoustic shadowing
May have mass-like appearance (tumefactive sludge)
– No vascularity on Doppler US and should be mobile
• Gallstones associated with older age, female gender, pregnancy, obesity, rapid weight loss, and medications
• Sludge associated with rapid weight loss, pregnancy, fasting, TPN, critical illnesses, and some medications
• Gallstones/sludge usually asymptomatic, but can be associated with biliary colic and numerous complications
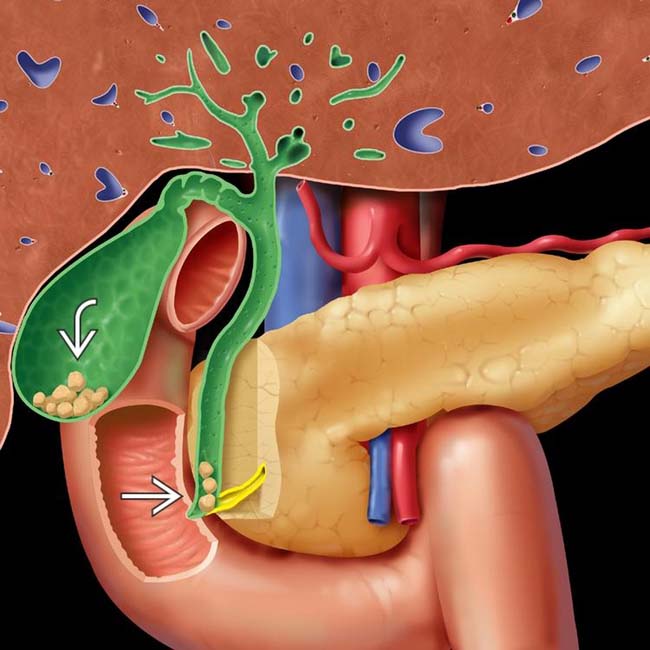
(Left) Coronal illustration shows cholelithiasis and choledocholithiasis . While most gallstones are asymptomatic, migration of stones to the cystic duct and common bile duct (CBD) may cause numerous complications, including biliary colic, cholecystitis, biliary obstruction, and pancreatitis.
(Right) Gross photograph shows a gallbladder (GB) filled with numerous smooth, yellow cholesterol stones. The GB wall is mildly thickened and hyperemic. (Courtesy G. F. Gray, MD.)
(Left) Gross photograph shows numerous faceted black pigment stones distending the GB lumen. The GB wall is thickened and edematous. (Courtesy G. F. Gray, MD.)
(Right) Grayscale ultrasound of the GB shows a typical echogenic stone within the GB lumen. Note the presence of posterior acoustic shadowing . The GB wall thickness is normal and there is no pericholecystic fluid to suggest cholecystitis.
• Gallstones: Concretions within biliary system (gallbladder [GB] and biliary ducts)
Cholesterol stone (75-80%): Cholesterol is main constituent
Pigment stone (20-25%): Calcium-bilirubinate is main constituent
– Black stone: Usually pigment stone in sterile GB; small and tar-like stones frequently associated with cirrhosis and hemolytic states
– Brown stone: Usually pigment stone in infected bile duct, associated with cholestasis and biliary infections (e.g., recurrent pyogenic cholangitis)
• Choledocholithiasis: Stones in common bile duct (CBD)
• Sludge: Suspension of particulate material/bile in GB
IMAGING
General Features
• Best diagnostic clue
Gallstone: Mobile, brightly echogenic mass in GB with marked posterior acoustic shadowing
Sludge: Mobile low-level echoes layering in dependent portion of GB with no acoustic shadowing
• Location
Cholesterol and black stones form within GB
Brown stones form within bile ducts
Small stones (either cholesterol or pigment) may pass into CBD
Stones usually found in dependent portion of GB
• Size
Cholesterol stones are often multiple and range up to several centimeters in diameter
Black stones are usually numerous and < 1.5 cm
Can fill GB with innumerable stones or 1 large stone
• Morphology
Surfaces of stones may be round or faceted
Rim calcification: Adsorbed rings of calcium in and on stone
Imaging Recommendations
• Best imaging tool
Ultrasound best for identifying GB stones
ERCP and MRCP superior for bile duct stones
• Protocol advice
Ultrasound harmonic imaging decreases side lobe, near field reverberation artifact
Radiographic Findings
• Only 10-20% of cholesterol stones have enough calcium to be visible on plain films
50-75% of black stones are radiopaque
Majority of brown stones are radiolucent
• Mercedes-Benz sign: Gas within central fissures of stones
Does not imply infection or complication
CT Findings
• No evidence that NECT improves visualization of stones
• Overall sensitivity of CT for stones is roughly 80%
20% of stones are not identified on CT, often “pure” cholesterol stones which are isodense to bile
Common duct stones difficult to perceive if located within nondilated duct
Higher kVp settings may improve stone visualization
• Single or multiple filling defects in GB or ducts
Density varies: Calcium density, soft tissue density, or lucent (pure cholesterol or gas-containing)
Pattern of calcification: Uniformly calcified, laminated, rim calcification, or central nidus of calcification
If stones not seen, “meniscus” configuration of distal CBD (with proximal dilatation) suggests occult stone
May be gas within stones on CT (Mercedes-Benz sign)
• Most helpful for assessing complications of gallstones, such as cholecystitis or gallstone ileus
• Sludge: Nonenhancing layering material with attenuation ≥ bile
Often not evident on CT (US is more sensitive)
MR Findings
• Stones most conspicuous on T2WI and MRCP
• Usually low signal (signal void) on T1WI and T2WI
May rarely show central hyperintensity on T1WI or T2WI due to presence of proteins within stones
May rarely have high T2 signal (bile within stone)
Pigment stones may sometimes show T1WI hyperintensity and are more variable in signal (on any sequence) compared to cholesterol stones
• MRCP superior to US or CT for identification of CBD stones
Accuracy probably equivalent to ERCP
Ultrasonographic Findings
• Gallstones
Ultrasound very sensitive (95%) and specific (95%) for stones > 2 mm
Brightly echogenic nodule in GB with marked posterior acoustic shadowing
– Small stones may not shadow
– Stones should be mobile when repositioning patient
– May show “twinkling” artifact on color Doppler images
Wall-echo-shadow sign when GB is filled with stones
– Anterior GB wall demarcated by echogenic line (wall), followed by layer of bile demarcated by hypoechoic line (echo), followed by posterior acoustic shadowing from superficial stones (shadow)
Only gold members can continue reading. Log In or Register to continue








 and choledocholithiasis
and choledocholithiasis  . While most gallstones are asymptomatic, migration of stones to the cystic duct and common bile duct (CBD) may cause numerous complications, including biliary colic, cholecystitis, biliary obstruction, and pancreatitis.
. While most gallstones are asymptomatic, migration of stones to the cystic duct and common bile duct (CBD) may cause numerous complications, including biliary colic, cholecystitis, biliary obstruction, and pancreatitis.


 within the GB lumen. Note the presence of posterior acoustic shadowing
within the GB lumen. Note the presence of posterior acoustic shadowing  . The GB wall thickness is normal and there is no pericholecystic fluid to suggest cholecystitis.
. The GB wall thickness is normal and there is no pericholecystic fluid to suggest cholecystitis.





















 Density varies: Calcium density, soft tissue density, or lucent (pure cholesterol or gas-containing)
Density varies: Calcium density, soft tissue density, or lucent (pure cholesterol or gas-containing) Pattern of calcification: Uniformly calcified, laminated, rim calcification, or central nidus of calcification
Pattern of calcification: Uniformly calcified, laminated, rim calcification, or central nidus of calcification If stones not seen, “meniscus” configuration of distal CBD (with proximal dilatation) suggests occult stone
If stones not seen, “meniscus” configuration of distal CBD (with proximal dilatation) suggests occult stone





 Wall-echo-shadow sign when GB is filled with stones
Wall-echo-shadow sign when GB is filled with stones







