Diet heavy in nitrites or nitrates; salted, smoked, poorly preserved food
CLINICAL ISSUES
• Most common signs/symptoms
Anorexia, weight loss, anemia, pain; can be asymptomatic
• Diagnosis by endoscopic biopsy and histology
DIAGNOSTIC CHECKLIST
• Image interpretation pearls
Can be ulcerative, polypoid, or infiltrative (scirrhous type) ± local and distant metastases
Beware of gastric fundus tumor simulating achalasia on esophagram
(Left) Graphic shows a large intraluminal mass with a broad base and irregular surface.
(Right) CECT in a 41-year-old woman shows mural thickening of soft tissue density , representing an infiltrative gastric carcinoma.
(Left) More cephalad section in the same patient shows circumferential thickening of the gastric wall that severely limits distensibility.
(Right) CT through the pelvis shows a collection of ascites and bilateral adnexal masses . The right adnexal mass is mostly cystic with a contrast-enhancing rim of soft tissue, while the left mass is more solid than cystic. At surgery, gastric carcinoma and bilateral ovarian metastases (Krukenberg tumors) were confirmed.
TERMINOLOGY
Definitions
• Malignancy arising from gastric mucosa
IMAGING
General Features
• Best diagnostic clue
Polypoid or circumferential mass with no peristalsis through lesion (at fluoroscopy)
• Morphology
Polypoid, ulcerated, infiltrative lesions
Fluoroscopic Findings
• Early (elevated, superficial, shallow)
Type 1: Elevated polypoid lesion protruding > 5 mm into lumen
Type 2: Superficial plaque-like lesion with mucosal nodularity/ulceration
Type 3: Shallow, irregular ulcer crater with adjacent nodular mucosa, clubbing/fusion/amputation of radiating folds
• 3 major fluoroscopic patterns on double-contrast upper GI series
Malignant ulcer
– Irregular ulcer crater
– Distortion or obliteration of surrounding areae gastricae
– Nodular, irregular, clubbed, or amputated folds that do not extend to edge of ulcer crater
– Ulcer does not project beyond expected contour of stomach (in profile)
Intraluminal mass
• Gastric cancers are often scirrhous
Those arising in antrum may cause gastric outlet obstruction
– Look for nodular thickened folds, absence of peristalsis
Linitis plastic (“leather bottle”)
– Small, nondistensible, nonperistaltic stomach
– Caused by diffuse infiltration of gastric wall
Pseudoachalasia:Gastric fundus carcinoma may invade distal esophagus and destroy myenteric plexus
– Resulting esophageal obstruction, dilated lumen, diminished peristalsis may be mistaken for primary achalasia
– Distinction: Look for nodular folds, mass in gastric fundus
• Advanced
Polypoid cancer can be lobulated or fungating
Lesion on dependent or posterior wall: Filling defect in barium pool
Lesion on nondependent or anterior wall: Etched in white by thin layer of barium trapped between mass and adjacent mucosa
Prolapsed polypoid antral carcinoma into duodenum: Filling defect in barium pool
Ulcerated carcinoma: 70% of all gastric cancers
• Malignant ulcer (in profile)
Intraluminal location within tumor
Tumor surrounding ulcer forms acute angle with gastric wall
Clubbed/nodular folds radiating to edge of ulcer crater
• Malignant ulcer (en face)
Irregular, scalloped, angular, stellate borders
Converging folds to ulcer: Blunted, nodular, clubbed, fused
Ulcer on nondependent/anterior wall: Double-ring shadow (edge of tumor and edge of ulcer)
Prone compression view: Filling of ulcer crater within discrete tumor on anterior wall
• Carman-Kirkland meniscus complex (lesser curvature antrum or body)
Broad, flat lesion; central ulceration, elevated margins
Prone compression view (mass on anterior wall): Radiolucent halo filling defect due to elevated edges; meniscoid ulcer-convex inner border, concave outer border
• Infiltrating: 5-15% of all gastric cancers
Irregular narrowing of stomach with nodularity and mucosal spiculation
May cause gastric outlet obstruction if advanced
• Scirrhous carcinoma (5-15%): Usually arise near pylorus, extend up
Linitis plastica (“leather bottle”): Irregular narrowing and rigidity
– Diffuse infiltration (nodularity, spiculation, ulceration, or thickened irregular folds)
Localized tumor: Short, annular lesion/shelf-like proximal borders in prepyloric region of antrum
CT Findings
• Primary tumor
• Negative contrast agents (water or gas) facilitate visualization of lesions
Polypoid mass ± ulceration
Focal wall thickening with mucosal irregularity or focal infiltration of wall
Ulceration: Gas-filled ulcer crater within mass
Infiltrating carcinoma: Wall thickening with loss of normal rugal fold pattern







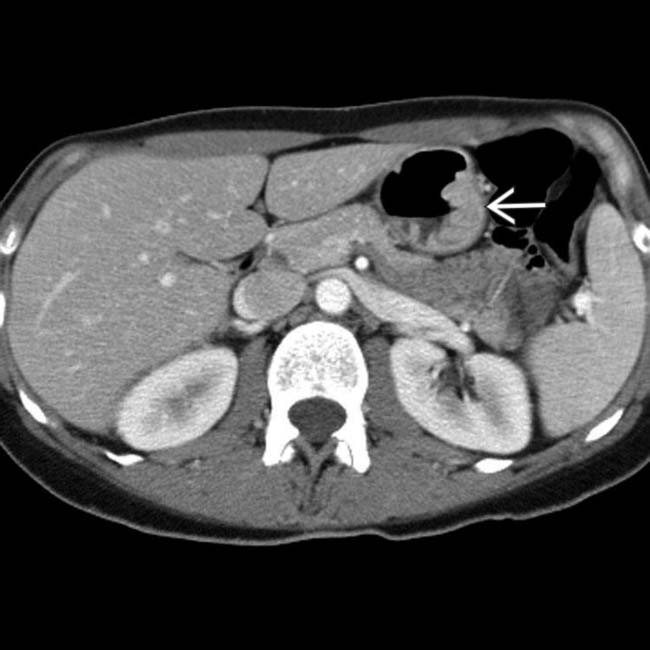
 , representing an infiltrative gastric carcinoma.
, representing an infiltrative gastric carcinoma.
 that severely limits distensibility.
that severely limits distensibility.
 and bilateral adnexal masses
and bilateral adnexal masses  . The right adnexal mass is mostly cystic with a contrast-enhancing rim of soft tissue, while the left mass is more solid than cystic. At surgery, gastric carcinoma and bilateral ovarian metastases (Krukenberg tumors) were confirmed.
. The right adnexal mass is mostly cystic with a contrast-enhancing rim of soft tissue, while the left mass is more solid than cystic. At surgery, gastric carcinoma and bilateral ovarian metastases (Krukenberg tumors) were confirmed.









 Lesion on nondependent or anterior wall: Etched in white by thin layer of barium trapped between mass and adjacent mucosa
Lesion on nondependent or anterior wall: Etched in white by thin layer of barium trapped between mass and adjacent mucosa

























 Krukenberg tumor: Metastases to ovaries via peritoneal seeding
Krukenberg tumor: Metastases to ovaries via peritoneal seeding 






