Common etiologies include Helicobacter pylori, NSAIDs, steroids, alcohol and coffee, stress
IMAGING
• Erosive gastritis, complete or varioliform erosions (most common type)
Erosions surrounded by radiolucent halos of edematous, elevated mucosa
Scalloped or nodular antral folds
Crenulation or irregularity of lesser curvature
Location: Gastric antrum on crests of rugal folds
Prolapse of antral mucosa through pylorus
Lack of complete distensibility of stomach (especially antrum)
• CT: Decreased wall attenuation (edema or inflammation)
Close to water density
• Upper GI series best for mucosal detail
CT for global view and concern for extragastric complications (e.g., perforation)
TOP DIFFERENTIAL DIAGNOSES
• Gastric carcinoma
• Zollinger-Ellison syndrome
• Acute pancreatitis
• Gastric metastases and lymphoma
DIAGNOSTIC CHECKLIST
• CT and upper GI usually suggest only gastritis
Specific etiology is determined by other medical data ± endoscopic biopsy
(Left) Graphic shows an ulcer crater and numerous mucosal erosions, mostly in the antrum along the ridges of hypertrophied folds. The antrum is less than completely distensible.
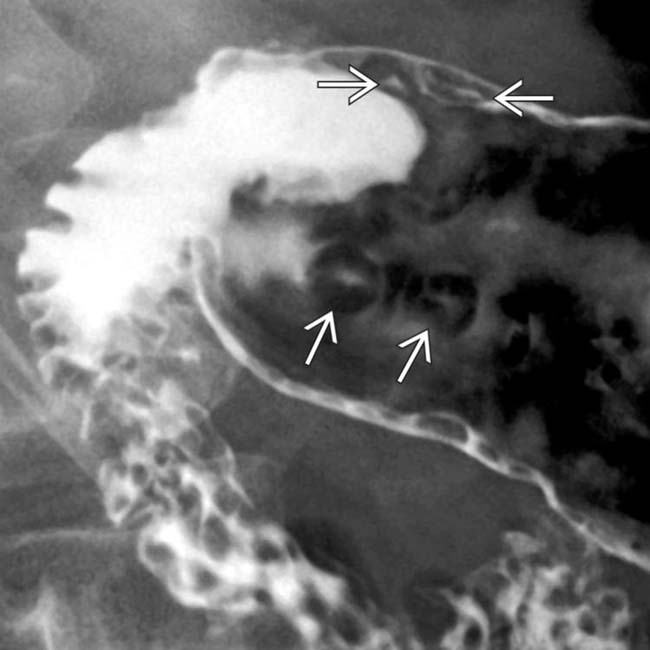
(Right) Upper GI series shows rows of varioliform erosions along the tops of hypertrophied gastric antral folds. This is diagnostic of gastritis but not specific as to the etiology.
(Left) CT of an athletic 30-year-old woman with severe abdominal pain and nausea due to NSAID gastritis shows massive thickening of the gastric wall with marked edema of the submucosa . The enhancing mucosa imparts a striped appearance to the gastric wall.
(Right) The body and antrum of the same patient are similarly involved . Following cessation of ibuprofen use and beginning antacid therapy, the patient’s symptoms resolved and a repeat CT scan (not shown) was normal.
TERMINOLOGY
Definitions
• Inflammation of gastric mucosa induced by group of disorders that differs in etiological, clinical, histological, and radiological findings
• Classification of gastritis
Erosive or hemorrhagic gastritis (2 types)
– Complete or varioliform
– Incomplete or “flat”
Antral gastritis
Helicobacter pylori gastritis
Hypertrophic gastritis
Atrophic gastritis (2 types: A and B)
Granulomatous gastritis (Crohn disease and tuberculosis)
Eosinophilic gastritis
Emphysematous gastritis
Caustic ingestion gastritis
Radiation gastritis
AIDS-related gastritis: Viral, fungal, protozoal, and parasitic infections
IMAGING
General Features
• Best diagnostic clue
Superficial ulcers and thickened folds
Upper GI Findings
• Erosive gastritis, complete or varioliform erosions (most common type)
Location: Gastric antrum on crests of rugal folds
Multiple punctate or slit-like collections of barium
Erosions surrounded by radiolucent halos of edematous, elevated mucosa
Scalloped or nodular antral folds
Epithelial nodules or polyps (chronic)
• Nonsteroidal anti-inflammatory drug (NSAID) induced
Linear or serpiginous erosions clustered in body, on or near greater curvature
Varioliform or linear erosions in antrum
NSAID-related gastropathy: Subtle flattening and deformity of greater curvature of antrum
• Antral gastritis
Thickened folds, spasm, or decreased distensibility
Scalloped or lobulated folds oriented longitudinally or transverse folds
Crenulation or irregularity of lesser curvature
Prolapse of antral mucosa through pylorus
• H. pylori gastritis
Location: Antrum, body, or occasionally fundus; diffuse or localized
Thickened, lobulated gastric folds
Enlarged areae gastricae (≥ 3 mm in diameter)
• Hypertrophic gastritis
Location: Fundus and body
Markedly thickened, lobulated gastric folds
• Atrophic gastritis
Narrowed, tubular, nondistensible stomach
Smooth, featureless mucosa, ↓ folds
Only gold members can continue reading. Log In or Register to continue










 along the tops of hypertrophied gastric antral folds. This is diagnostic of gastritis but not specific as to the etiology.
along the tops of hypertrophied gastric antral folds. This is diagnostic of gastritis but not specific as to the etiology.
 . The enhancing mucosa imparts a striped appearance to the gastric wall.
. The enhancing mucosa imparts a striped appearance to the gastric wall.
 . Following cessation of ibuprofen use and beginning antacid therapy, the patient’s symptoms resolved and a repeat CT scan (not shown) was normal.
. Following cessation of ibuprofen use and beginning antacid therapy, the patient’s symptoms resolved and a repeat CT scan (not shown) was normal.




































