• MR shows some elements better than CT (lipid and hemorrhage)
• Gadoxetate-enhanced MR (Eovist; Primovist)
Adenoma shows no substantial uptake or retention
Key distinction from FNH
• T1WI: Mass: Heterogeneous signal intensity
Increased signal intensity (due to fat or recent hemorrhage)
Decreased signal intensity (necrosis, calcification, old hemorrhage)
• Heterogeneous, hypervascular mass with foci of fat or hemorrhage in a young woman
TOP DIFFERENTIAL DIAGNOSES
• Hepatocellular carcinoma (HCC)
HCC typically occurs in older, cirrhotic men
• Fibrolamellar HCC
• Focal nodular hyperplasia
Homogeneously enhances; retains gadoxetate
• Hypervascular metastases
PATHOLOGY
• Hepatic steatosis, pregnancy, anabolic steroids, and oral contraceptives increase number and growth rate of adenomas
CLINICAL ISSUES
• Risk factors for HCC
Large adenoma, male sex, glycogen storage disease, anabolic steroid use, CTNNB1 -mutated subtype of HA
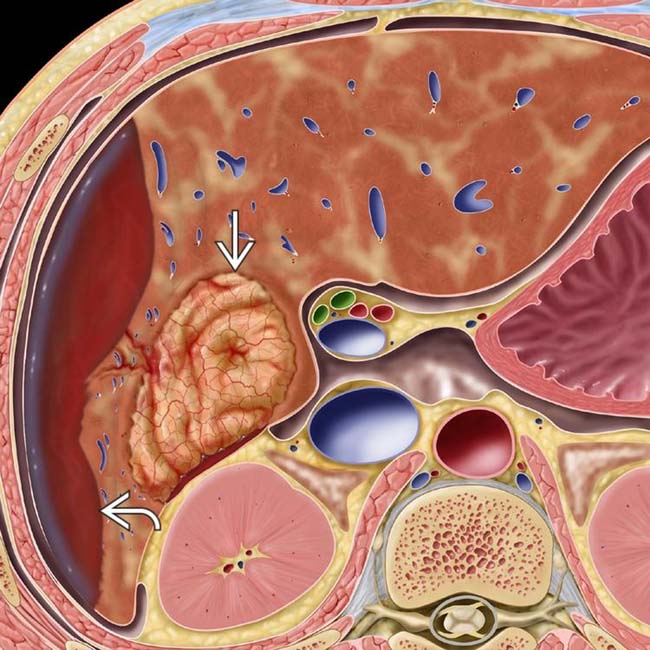
(Left) Graphic shows a hypervascular mass in the right lobe and spontaneous subcapsular bleeding .
(Right) Axial CECT of a 40-year-old woman with sudden RUQ pain and syncope shows an intensely enhancing mass in the right lobe of the liver. A lentiform heterogeneous collection of fluid indents the surface of the liver, and within this collection is a focus of higher density likely representing a sentinel clot. A ruptured inflammatory hepatic adenoma was resected.
(Left) Photograph of a resected specimen shows a large adenoma with central areas of rupture and hemorrhage . (Courtesy M. Yeh, MD, PhD.)
(Right) Photomicrograph of a hepatic adenoma features a thin-walled unpaired vessel surrounded by neoplastic hepatocytes with abundant steatosis. Imaging often reveals these features, directly or indirectly. (Courtesy M. Yeh, MD, PhD.)
TERMINOLOGY
Abbreviations
• Hepatic adenoma (HA)
Synonyms
• Hepatocellular adenoma, liver cell adenoma
Definitions
• Heterogeneous group of benign hepatocellular neoplasms with distinctive genetic, pathologic, and clinical features
IMAGING
General Features
• Best diagnostic clue
Heterogeneous, hypervascular mass with foci of fat or hemorrhage in a young woman
• Location
Subcapsular region of right lobe of liver (75%)
Intraparenchymal or pedunculated (10%)
• Size
Varies from 6-30 cm
• Key concepts
Very uncommon relative to focal nodular hyperplasia (FNH) and hepatocellular carcinoma (HCC)
3 distinct subtypes with different genetics, pathology, clinical features
CT Findings
• Depending on HA subtype
Encapsulation seen in ∼ 20%, best on delayed phase CECT
Hemorrhage within tumor, best seen on NECT as hyperdense foci
Intratumoral lipid, best seen on NECT as hypodense foci
Hypervascularity
– Most intense and persistent in inflammatory subtype of HA
Calcification: Focal, present in ∼ 5%
MR Findings
• T1WI
Mass: Heterogeneous signal intensity
– Increased signal intensity (due to fat and recent hemorrhage), more evident on MR than CT
– Decreased signal intensity (necrosis, calcification, old hemorrhage)
Rim (fibrous pseudocapsule): Hypointense
• T2WI
Mass: Heterogeneous signal intensity
– Increased signal intensity (old hemorrhage, necrosis)
– Decreased signal intensity (fat, recent hemorrhage)
Rim (fibrous pseudocapsule): Hypointense
• T1WI C+
Gadolinium, arterial phase
– Heterogeneous hypervascular enhancement (especially in inflammatory subtype)
Delayed phase
– Pseudocapsule: Hyperintense to liver and adenoma
• Gadoxetate-enhanced MR (Eovist, Primovist)
Hepatocellular-specific contrast agent
Adenoma shows no substantial uptake or retention on delayed imaging
– Key distinction from FNH
Ultrasonographic Findings
• Grayscale ultrasound
Complex, hyper-/hypoechoic, heterogeneous mass with anechoic areas
– Due to fat, hemorrhage, necrosis, and calcification
– Capsule may be seen
• Color Doppler
Hypervascular tumor
Large peripheral arteries and veins
Intratumoral veins present
– Absent in FNH; useful distinction for adenoma
Angiographic Findings
• Conventional
Hypervascular mass with centripetal flow
Enlarged hepatic artery with feeders at tumor periphery (50%)
Hypovascular; avascular regions
– Due to hemorrhage and necrosis
Nuclear Medicine Findings
• Technetium sulfur colloid (TcSC)
Usually “cold” (photopenic) (80%)
Uncommonly “warm” (20%)
– Due to uptake in sparse Kupffer cells
• HIDA scan
Increased activity in some
• Gallium scan
No uptake
Imaging Recommendations
• Best imaging tool
Gadoxetate-enhanced MR, including multiphasic and delayed imaging
In- and opposed-phase GRE
DIFFERENTIAL DIAGNOSIS
Hepatocellular Carcinoma
• May be hard to distinguish on imaging or pathology
• Biliary, vascular, nodal invasion and metastases = malignancy
• HCC typically occurs in older, cirrhotic men
Adenoma occurs in young, healthy women
Fibrolamellar HCC
• Large, lobulated mass with scar and septa
• Vascular, biliary invasion and metastases common
Focal Nodular Hyperplasia
• Arterial phase: Homogeneously enhancing mass
Only gold members can continue reading. Log In or Register to continue








 in the right lobe and spontaneous subcapsular bleeding
in the right lobe and spontaneous subcapsular bleeding  .
.
 in the right lobe of the liver. A lentiform heterogeneous collection of fluid indents the surface of the liver, and within this collection is a focus of higher density
in the right lobe of the liver. A lentiform heterogeneous collection of fluid indents the surface of the liver, and within this collection is a focus of higher density  likely representing a sentinel clot. A ruptured inflammatory hepatic adenoma was resected.
likely representing a sentinel clot. A ruptured inflammatory hepatic adenoma was resected.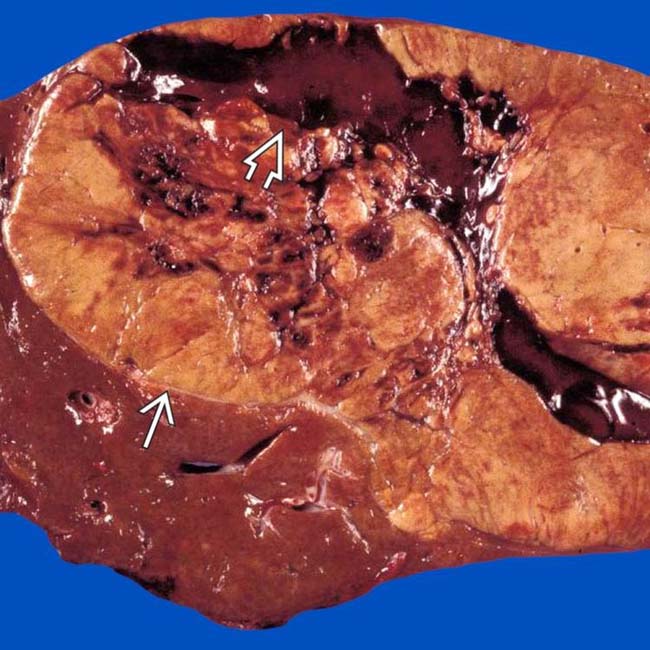
 with central areas of rupture and hemorrhage
with central areas of rupture and hemorrhage  . (Courtesy M. Yeh, MD, PhD.)
. (Courtesy M. Yeh, MD, PhD.)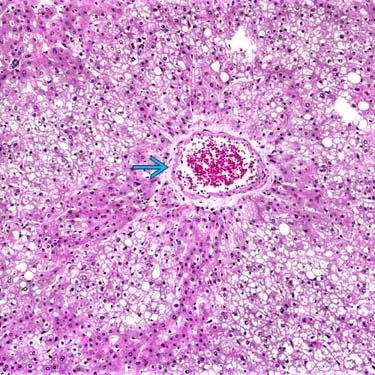
 surrounded by neoplastic hepatocytes with abundant steatosis. Imaging often reveals these features, directly or indirectly. (Courtesy M. Yeh, MD, PhD.)
surrounded by neoplastic hepatocytes with abundant steatosis. Imaging often reveals these features, directly or indirectly. (Courtesy M. Yeh, MD, PhD.)





































