When > 10, consider autosomal dominant polycystic liver disease (ADPLD) or biliary hamartomas
• Sharply defined margins, thin walls
• Water density (-10 to +10 HU)
• Usually no or few thin septations
No mural nodularity or wall calcification
• Hemorrhage into cyst may simulate tumor
No enhancement of “solid” material
Varied MR signal intensity (due to mixed blood products)
• US: Anechoic mass, accentuated through transmission
Smooth borders; thin or invisible wall
• Size varies from few mm to > 20 cm
Rarely are the cysts of similar size
Helps to differentiate from biliary hamartomas, which are all usually < 15 mm
TOP DIFFERENTIAL DIAGNOSES
• AD polycystic disease, liver
• Cystic or necrotic metastases
• Biliary cystadenocarcinoma
• Biliary hamartomas
• Ciliated hepatic foregut cyst
• Hepatic cavernous hemangioma
• Biloma
• Hepatic pyogenic abscess
• Hydatid (echinococcal) disease
DIAGNOSTIC CHECKLIST
• Sonography shows cyst morphology better than CT
(Left) Axial CECT shows a spherical hepatic mass with water density and homogeneous contents. No internal debris or wall irregularities are present. This is a classic simple cyst.
(Right) Ultrasound in the same patient shows an anechoic mass with accentuated through-transmission . Either CT or US would have been sufficient to establish the diagnosis in this patient.
(Left) Axial T1WI MR shows a large, cystic, hepatic mass that has homogeneous low intensity and several thin septa .
(Right) Coronal T2WI shows uniform high intensity and septa . The cyst has remained stable for years, and no other evaluation or intervention was performed.
TERMINOLOGY
Synonyms
• Simple hepatic or bile duct cyst
Definitions
• Benign, congenital, developmental lesion derived from biliary endothelium
IMAGING
General Features
• Best diagnostic clue
Anechoic lesion with increased through-transmission and no mural nodularity on US
• Location
Any location within liver
• Size
Varies from few mm to > 20 cm
– Rarely are the cysts of similar size
– Helps to differentiate from biliary hamartomas, which are all usually < 15 mm
• Morphology
Spherical or oval, well marginated
• Key concepts
Classified based on etiology and pathogenesis
Congenital or developmental: Simple hepatic or bile duct cyst
– Often multiple: Usually < 10
– No communication with bile ducts
When > 10 in number, fibropolycystic disease must be considered







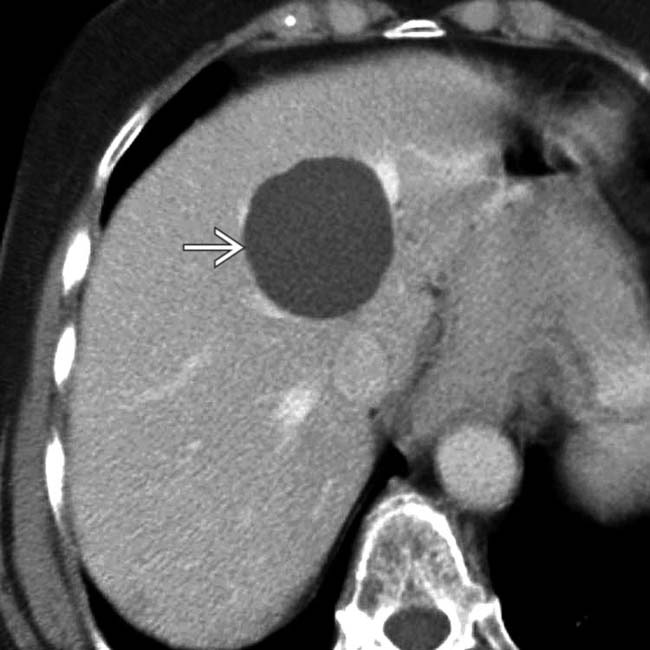
 with water density and homogeneous contents. No internal debris or wall irregularities are present. This is a classic simple cyst.
with water density and homogeneous contents. No internal debris or wall irregularities are present. This is a classic simple cyst.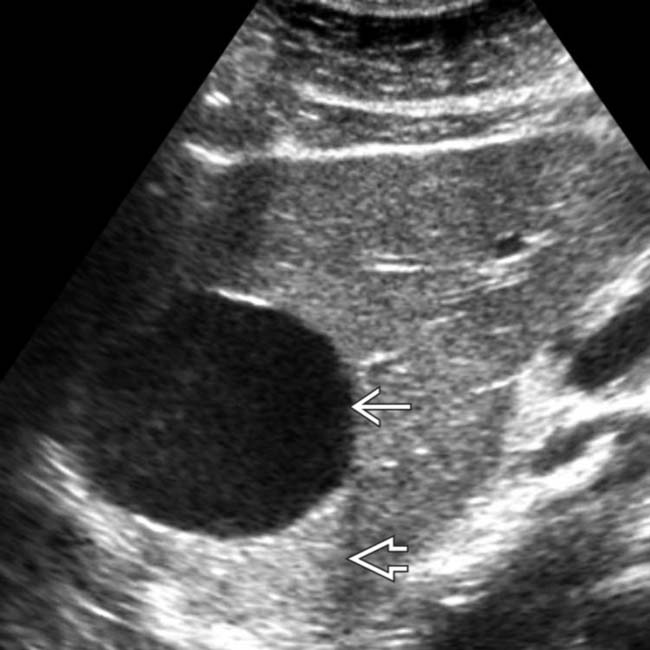
 with accentuated through-transmission
with accentuated through-transmission  . Either CT or US would have been sufficient to establish the diagnosis in this patient.
. Either CT or US would have been sufficient to establish the diagnosis in this patient.
 that has homogeneous low intensity and several thin septa
that has homogeneous low intensity and several thin septa  .
.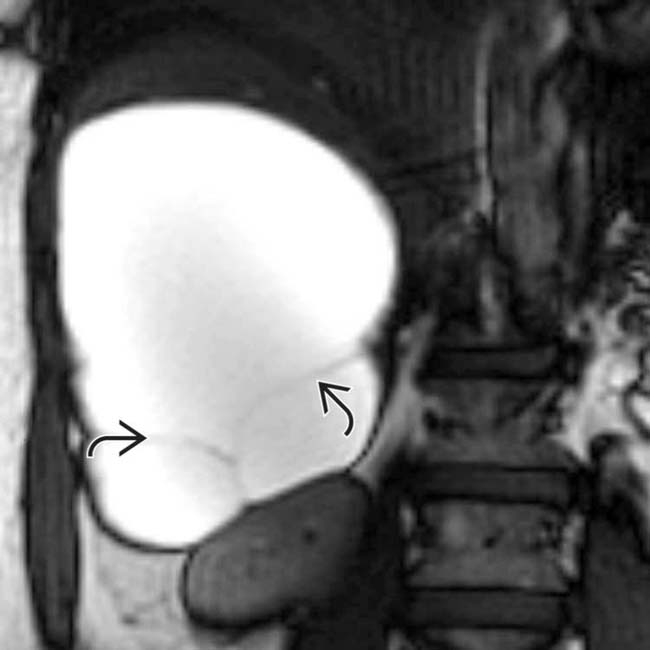
 . The cyst has remained stable for years, and no other evaluation or intervention was performed.
. The cyst has remained stable for years, and no other evaluation or intervention was performed.


























