Gadolinium enhancement required to detect very small lesions
TOP DIFFERENTIAL DIAGNOSES
• Metastases
• Lymphomatous/leukemic foci in liver
• Biliary hamartomas
• Caroli disease
PATHOLOGY
• Originates from intestinal seeding of portal venous circulation
• Candida albicans: Most common cause of fungal microabscesses
CLINICAL ISSUES
• Most common signs/symptoms
Asymptomatic or abdominal pain and fever
Erythematous papules on skin
• Clinical profile: Immunocompromised patient recovering from neutropenia
High incidence in transplant patients with fungal colonization
DIAGNOSTIC CHECKLIST
• Rule out other innumerable hypodense liver lesions
• Biopsy specimen for histology/microbiology
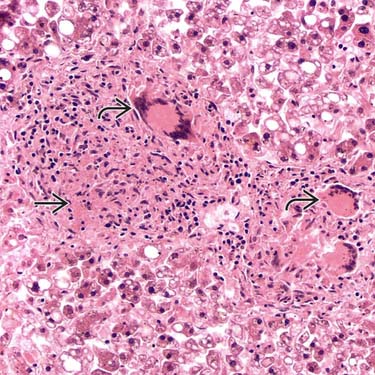
(Left) High-power view of hepatic miliary tuberculosis shows a granuloma with focal eosinophilic granular necrotic material and several multinucleated giant cells . (Courtesy J. Misdraji, MD.)
(Right) Axial CECT of a woman with breast cancer, fever, and liver dysfunction demonstrates multiple small, low-density lesions due to hepatic candidiasis. Metastases would uncommonly be so numerous and small.
(Left) Axial CECT in a patient undergoing chemotherapy for acute leukemia, now presenting with a fever, demonstrates fungal abscesses due to Candida. Note the multiple small (< 1 cm) lesions in all lobes of the liver.
(Right) Axial CECT of a 33-year-old woman with non-Hodgkin lymphoma presenting with a recent spike in temperature shows innumerable tiny hypodense lesions in the liver and spleen due to candidiasis. Lymphomatous parenchymal involvement is rarely detected as such small discrete lesions.
TERMINOLOGY
Definitions
• Opportunistic infection of liver (± other viscera), usually by fungal or mycobacterial organisms
IMAGING
General Features
• Best diagnostic clue
Multiple well-defined, rounded microabscesses in liver
• Location
May involve multiple organs
– Liver, spleen, kidneys, lungs
• Size
Microabscesses < 2 cm
• Morphology
Spherical with complex fluid center, ± enhancing capsule
CT Findings
• NECT
Multiple small, hypodense lesions
± scattered areas of calcific density (healing phase)
• CECT
Biphasic CT may be more accurate than venous phase only
– Nonenhancing hypodense centers
– ± peripheral rim enhancement
Central or eccentric “dot” felt to represent hyphae
Rarely may demonstrate unusual central enhancement on arterial phase with double peripheral rim




 and several multinucleated giant cells
and several multinucleated giant cells  . (Courtesy J. Misdraji, MD.)
. (Courtesy J. Misdraji, MD.)
 due to hepatic candidiasis. Metastases would uncommonly be so numerous and small.
due to hepatic candidiasis. Metastases would uncommonly be so numerous and small.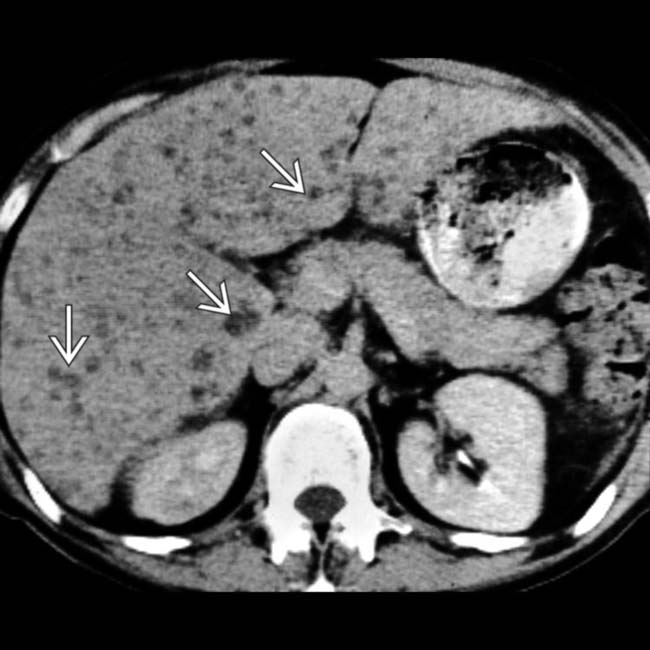
 in all lobes of the liver.
in all lobes of the liver.






























