No reliable imaging findings to suggest or confirm diagnosis
• Biliary leak
From entry of T tube: Easily treated
From biliary anastomosis: Requires revision
From intrahepatic ducts: Biliary necrosis; catastrophic
• Biliary obstruction
Balloon dilation and stenting
• Hepatic artery stenosis
Damped waveform in hepatic artery distal to stenosis: Slow systolic upstroke; decreased resistive index (< 0.5)
Narrowing at hepatic artery anastomosis with turbulent flow, focally ↑ velocity (> 0.3 m/s)
CT (or MR) angiography for detailed analysis
• Hepatic artery thrombosis
Accompanied by biliary necrosis; catastrophic
• Hepatic arterial pseudoaneurysm
From biopsy or surgical error
• Portal vein stenosis
Uncommon: Treated by angioplasty and stent
• IVC anastomotic stenosis
Can be suggested by US (anastomotic narrowing, turbulent, rapid flow across anastomosis), CT, or MR
• Recurrent disease within allograft
Primary sclerosing cholangitis: Tends to recur
Hepatocellular carcinoma
Recurrent viral hepatitis or primary biliary cirrhosis
• Extrahepatic complications
Abdominal fluid collections
Post-transplant lymphoproliferative disorder
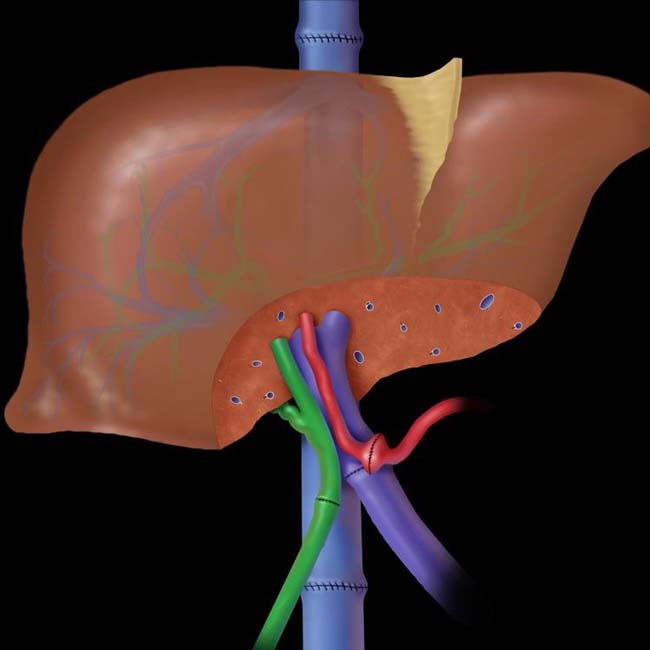
(Left) Graphic shows the typical anatomy for whole liver transplantation. Some liver is cut away to show anastomoses more clearly, as there are a number of common variations for vascular and biliary anastomoses.
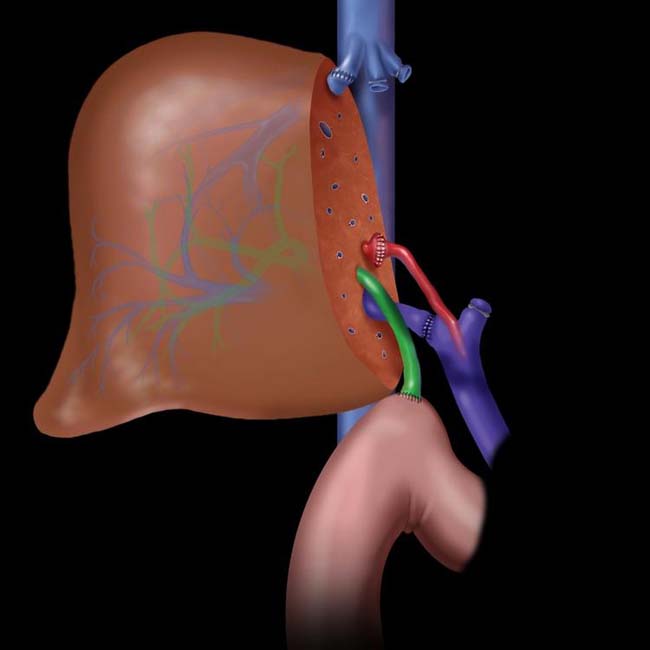
(Right) Graphic shows the typical anatomy of an adult partial-liver recipient (living donor). Note the biliary-enteric anastomosis to a Roux limb. Complications are more common than for whole liver allografts due to the many transected vessels and ducts and the small size of the structures for anastomosis.
(Left) Axial CECT shows a “halo” of low density surrounding some of the portal veins. This is a typical feature of periportal lymphedema, which is common and of no clinical concern in the early post-transplantation setting.
(Right) T-tube cholangiogram shows a mild waist-like narrowing at the biliary anastomosis without dilation of the upstream bile ducts. This is the normal appearance of a duct-to-duct anastomosis.
TERMINOLOGY
Definitions
• Whole liver allograft (cadaver donor)
Orthotopic liver transplantation (OLT)
Included from donor
– Intact inferior vena cava (IVC)
Anastomosed end-to-end or as “piggy-back” side-to-side
– Hepatic artery (HA)
Anastomosed end-to-end, sometimes with aortic (Carrel) patch
– Portal vein (PV)
End-to-end anastomosis
– Bile duct
Anastomosed end-to-end with recipient duct (70%) or to Roux limb
• Cadaver split liver (2 halves to separate recipients)
Right lobe to adult recipient (IVC, HA, PV, bile duct)
Left lobe to child recipient (complex anastomoses)
• Living donor transplant
Child recipient: Generally receives lateral segment of donor liver
Adult recipient: Receives right lobe of donor
Complex biliary and vascular anastomoses
IMAGING
Normal Post-Transplantation Findings
• Right pleural effusion (usually resolves spontaneously)
• Right adrenal hematoma
Adrenal veins injured or ligated during OLT
No clinical importance
• Periportal lymphedema
Lucent “halo” around PVs and IVC
No significance; resolves spontaneously
• Vascular and biliary anastomoses may show waist-like narrowing
Should not have functional narrowing
Normal indices on US: Hepatic artery
– Resistive index (RI): 0.5-0.7
– Rapid systolic acceleration time (< 80 ms)
– Flow velocity at anastomosis < 200-300 cm/s
Portal vein
– Mild phasicity with respiration; no turbulent flow
Hepatic veins (HV), IVC
– Triphasic waveforms reflective of cardiac contractility
• Biliary anastomosis
Waist-like narrowing without dilation of upstream ducts
Duct-duct anastomosis may be stented with T tube for several months
– Allows access for cholangiography
Performed in early post-OLT and repeated as indicated
• Liver parenchyma
Normal texture by all imaging modalities
Partial liver recipients
– Liver grows to near normal volume within months
Pre-Transplantation Evaluation
• Imaging and clinical evaluation of severity of cirrhosis and portal hypertension
Size and morphology of liver
Ascites, splenomegaly, extent of varices
Presence and stage of hepatocellular carcinoma (HCC)
– Size, number, presence of vascular invasion, extrahepatic spread
– Early stage HCC may be good candidate for transplantation (receives increased MELD points)
Model for end-stage liver disease (MELD)
– Based on etiology of cirrhosis, plus serum creatinine, bilirubin, and International Normalised Ratio (INR)
• Detailed evaluation of hepatic vessels
Note any anomalies (e.g., “replaced” HA)
– Check for severe atherosclerosis, median arcuate ligament compression of celiac axis
PV: Check for thrombosis, mural calcification, diminutive size
HVs: Check for thrombosis (Budd-Chiari)
Allograft Rejection
• No reliable imaging findings to suggest or confirm diagnosis
• Clinical suspicion leads to US-guided biopsy of allograft
US is best modality for guidance
– Safest, least expensive, least discomfort
Biliary Complications
• Biliary leak
Leak from entry of T tube
– Often encountered after removal of T tube after several months
– Recognized by cholangiography, biliary scintigraphy, or aspiration of fluid collection identified by US or CT
– Easily confirmed by ERCP and treated by placement of temporary biliary stent
Leak from biliary anastomosis
– Usually due to surgical error
– Often requires surgical revision of anastomosis
Leak from intrahepatic ducts
– May be due to biopsy (resolves spontaneously)
– Usually due to biliary necrosis
Result of HA stenosis or thrombosis
– Usually requires retransplantation in adults
Strictures or irregularity of intrahepatic ducts
– Nonspecific
– Possible etiologies include incomplete distention (artifact), infection, rejection, ischemia, recurrent primary sclerosing cholangitis




 Damped waveform in hepatic artery distal to stenosis: Slow systolic upstroke; decreased resistive index (< 0.5)
Damped waveform in hepatic artery distal to stenosis: Slow systolic upstroke; decreased resistive index (< 0.5)












 without dilation of the upstream bile ducts. This is the normal appearance of a duct-to-duct anastomosis.
without dilation of the upstream bile ducts. This is the normal appearance of a duct-to-duct anastomosis.































 Leak from entry of T tube
Leak from entry of T tube






 Anastomotic
Anastomotic





