75% of stomach is removed by dividing stomach along its long axis
– Complications: Less or comparable to LAGB, less than Roux-en-Y gastric bypass (RYGB)
– Leak: Early complication seen in < 1%
– Stricture in mid stomach (transient or persistent)
• RYGB procedure
Gastrointestinal complications occur in ∼ 10%
Anastomotic stricture
– Dilatation of gastric pouch, spherical shape, air-fluid-contrast material levels, delayed emptying
Anastomotic leaks
– Most commonly at gastrojejunal anastomosis
– CT may demonstrate major and minor leaks; fluid collections not evident on upper GI series
Marginal ulcers; rate of 0.5-1.4% after RYGB
– Usually result of ischemia
Small bowel obstruction (SBO)
– Most common etiology: Internal hernias (IH) and adhesions
– IH: CT appearance depends on location
– Clustering of SB loops; congestion, crowding, twisting of mesenteric vessels
Obstruction of excluded stomach and biliopancreatic limb
– Cannot be diagnosed with upper GI series; CT is key
– May progress to perforation (often fatal)
• CT and upper GI radiography have complementary roles
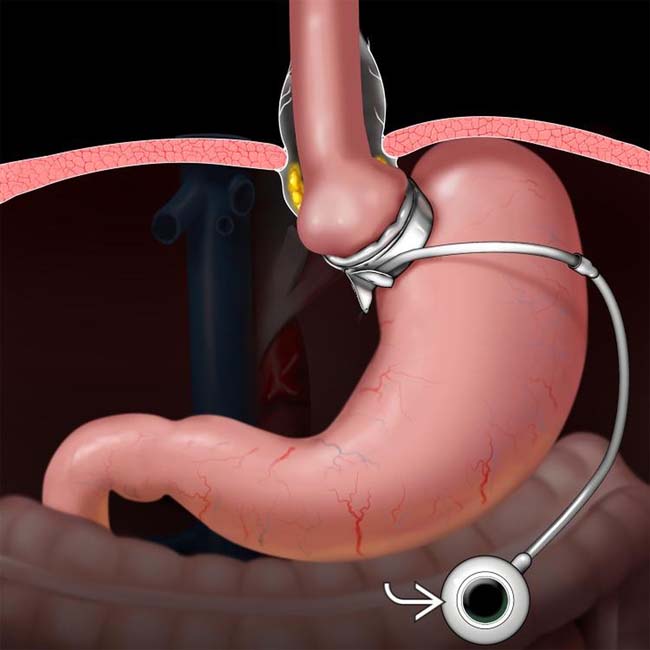
(Left) Graphic depicts the gastric banding procedure in which a silicone band is looped around the proximal stomach. A tube connects the inflatable liner of the band to a subcutaneously placed port that can be accessed and inflated or deflated with injections of fluid.
(Right) Spot film from an esophagram shows the gastric band in its expected position with a “Phi” angle of ∼ 45° (normal). The dilated, slowly emptying esophagus indicates that the band is too tight and fluid will be removed from the access port .
(Left) Radiograph shows an abnormal position of the gastric band , which has slipped inferiorly and rotated clockwise. The connecting tubing has also migrated into a more rightward position than expected.
(Right) An upright film from an esophagram in the same patient shows dilation of a larger than expected portion of the proximal stomach with air-fluid-contrast levels, indicating stasis. Slip and rotation of the band often result in obstruction and require revision.
TERMINOLOGY
Definitions
• Imaging techniques and findings used to evaluate possible complications of surgical procedures meant to induce weight loss









 that can be accessed and inflated or deflated with injections of fluid.
that can be accessed and inflated or deflated with injections of fluid.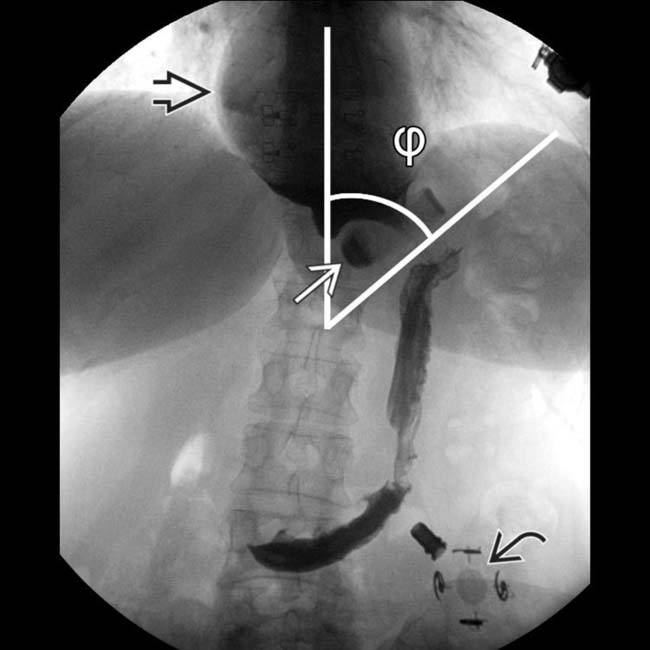
 in its expected position with a “Phi” angle of ∼ 45° (normal). The dilated, slowly emptying esophagus
in its expected position with a “Phi” angle of ∼ 45° (normal). The dilated, slowly emptying esophagus  indicates that the band is too tight and fluid will be removed from the access port
indicates that the band is too tight and fluid will be removed from the access port  .
.
 , which has slipped inferiorly and rotated clockwise. The connecting tubing
, which has slipped inferiorly and rotated clockwise. The connecting tubing  has also migrated into a more rightward position than expected.
has also migrated into a more rightward position than expected.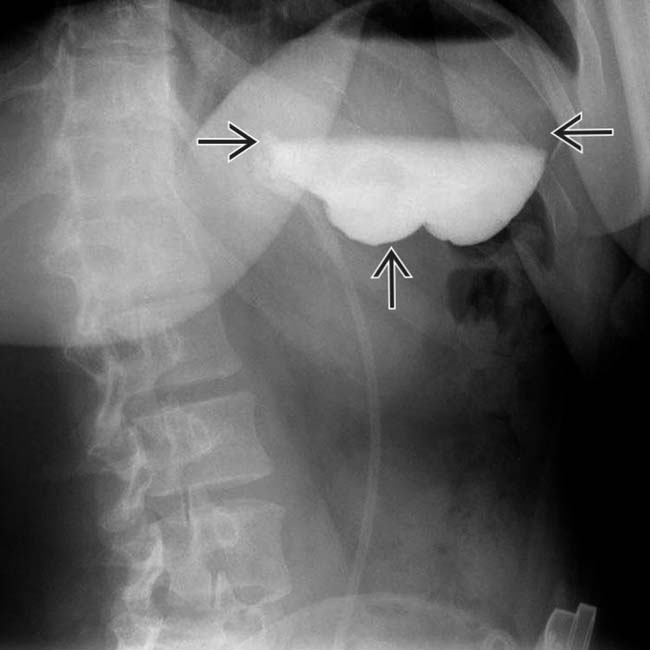
 with air-fluid-contrast levels, indicating stasis. Slip and rotation of the band often result in obstruction and require revision.
with air-fluid-contrast levels, indicating stasis. Slip and rotation of the band often result in obstruction and require revision. Laparoscopic adjustable gastric banding (LAGB) procedure
Laparoscopic adjustable gastric banding (LAGB) procedure Sleeve gastrectomy (gastric sleeve)
Sleeve gastrectomy (gastric sleeve) Laparoscopic Roux-en-Y gastric bypass procedure (RYGB)
Laparoscopic Roux-en-Y gastric bypass procedure (RYGB)
 Should lie at a “phi” angle (between vertical line and horizontal axis of band) between 30 and 60 degrees
Should lie at a “phi” angle (between vertical line and horizontal axis of band) between 30 and 60 degrees




































 “B” = biliopancreatic limb (excluded stomach, duodenum, and proximal jejunum)
“B” = biliopancreatic limb (excluded stomach, duodenum, and proximal jejunum)










