Hypotensive episodes: Hemorrhagic, cardiogenic, or septic shock
CHF, arrhythmia, drugs (e.g., digitalis), trauma
CLINICAL ISSUES
• Major predisposing cause in elderly: Nonocclusive vascular disease (hypoperfusion)
Most common cause of colitis in elderly, often self-limiting
• Presentation: Bloody diarrhea, hypotension
(Left) Graphic shows luminal narrowing and wall thickening near the splenic flexure, a “watershed” area between the vascular distribution of the SMA and IMA.
(Right) This 89-year-old man had pain and bloody diarrhea several hours after a hip arthroplasty procedure. Coronal reformatted CECT shows wall thickening and mucosal and mesenteric hyperemia affecting the descending colon . Incidental renal allograft noted .
(Left) Axial CECT in the same case shows submucosal edema and luminal narrowing of the descending colon . The SMA and SMV are patent.
(Right) Another CT section in this patient shows wall thickening and pericolonic stranding of the descending colon , whereas the remaining colon is normal. The rectum (not shown) was normal. These are classic clinical and CT features of ischemic colitis due to a hypotensive episode in an elderly patient.
TERMINOLOGY
Definitions
• Compromise of mesenteric blood supply leading to colonic injury
IMAGING
General Features
• Best diagnostic clue
Symmetric, long segmental colonic wall thickening on CT
Pneumatosis, mesenteric venous gas; more definitive but less common findings
• Location
Watershed segments of colon
Radiographic Findings
• Radiography
Supine abdominal films
– Normal or nonspecific ileus
– “Thumbprinting” (submucosal edema or hemorrhage)
– Luminal narrowing or transverse ridging (spasm)
Fluoroscopic Findings
• Barium enema
Hallmark: Serial change on studies performed over days, weeks, or months
“Thumbprinting”
– Usually within 24 hours after onset
– Thickened, nodular transverse folds (submucosal edema or hemorrhage)
– Most consistent and characteristic finding (75% of cases)
Ulceration: Mucosal sloughing
– Usually 1-3 weeks after onset
– Longitudinal or discrete, superficial or deep, small or large collections of barium
Stricture: 12% of cases heal with stricture formation
Intramural barium: Rare, due to sloughing of necrotic mucosa











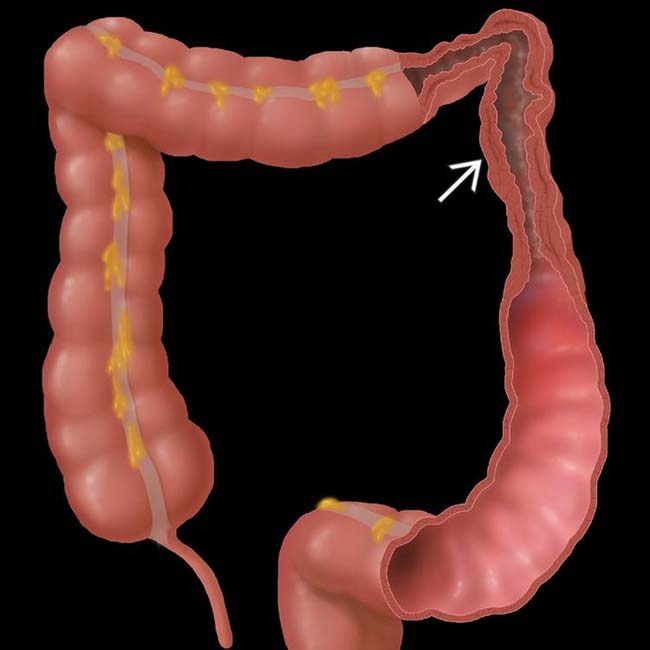
 near the splenic flexure, a “watershed” area between the vascular distribution of the SMA and IMA.
near the splenic flexure, a “watershed” area between the vascular distribution of the SMA and IMA.
 . Incidental renal allograft noted
. Incidental renal allograft noted  .
.
 . The SMA and SMV are patent.
. The SMA and SMV are patent.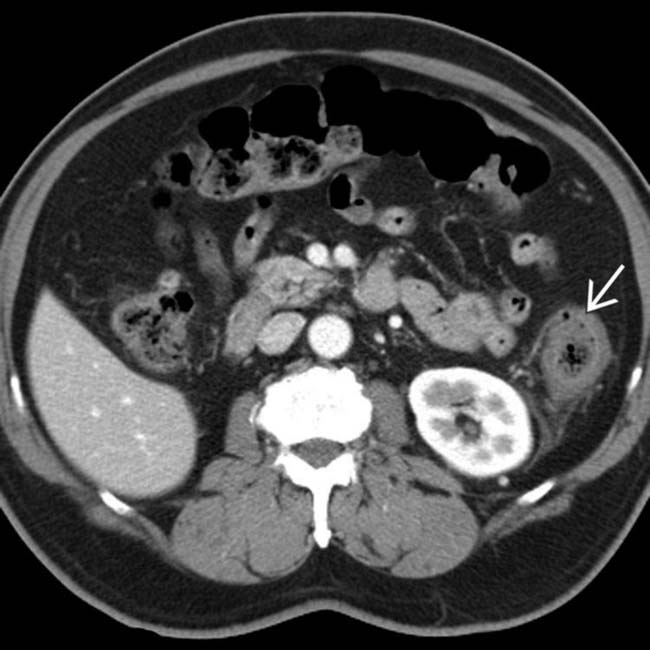
 , whereas the remaining colon is normal. The rectum (not shown) was normal. These are classic clinical and CT features of ischemic colitis due to a hypotensive episode in an elderly patient.
, whereas the remaining colon is normal. The rectum (not shown) was normal. These are classic clinical and CT features of ischemic colitis due to a hypotensive episode in an elderly patient.












 Hypoperfusion ischemia
Hypoperfusion ischemia












