Polygonal fluid collections between folds of mesentery, bowel loops
Indicates bowel &/or mesenteric injury
• Active bleeding = isodense with enhanced vessels
• Extraluminal gas: Intra- or retroperitoneal air
May be absent even with transmural lacerations
• Seat belt sign: Infiltration or hematoma in subcutaneous fat of lower anterior abdominal wall
• Free fluid without an apparent solid organ injury
Larger amounts, especially of blood attenuation (> 35 HU) are due to trauma
Look carefully for mesenteric, bowel, or solid visceral injury
TOP DIFFERENTIAL DIAGNOSES
• “Shock bowel”
• Coagulopathy (intramural hematoma)
• Vasculitis
PATHOLOGY
CLINICAL ISSUES
• Bowel and mesenteric injuries are found in 2-5% of patients taken to surgery after abdominal trauma
• Active mesenteric bleeding requires surgery
• Use of seat belt restraints has decreased mortality from motor vehicle crash
Incidence of bowel and mesenteric injuries has increased
DIAGNOSTIC CHECKLIST
• Check for mechanism of injury
• Don’t succumb to satisfaction of search
• Solid visceral injuries are often more obvious, but less important than injuries to bowel or mesentery
• CT is much more accurate in diagnosis of bowel injury from blunt trauma as opposed to penetrating trauma (e.g., stab wound to the abdomen)
(Left) Axial CECT in a 24-year-old man injured in a motor vehicle crash (MVC) shows a sentinel clot , adjacent to thick-walled jejunum, and active bleeding, as evidenced by the contrast extravasation . All characteristic findings in intestinal trauma.
(Right) Coronal CECT in the same patient shows an injured branch of the superior mesenteric artery with a large focus of contrast extravasation . The mesenteric injury was surgically repaired and a segment of small intestine was resected.
(Left) Axial CECT in a 28-year-old man who was injured in an MVC demonstrates ectopic gas adjacent to a thick-walled jejunal segment , indicative of transmural laceration or perforation.
(Right) Axial CECT in the same patient demonstrates mesenteric stranding , a characteristic finding in the setting of intestinal trauma.
TERMINOLOGY
Definitions
• Injury to mesentery &/or small intestine
IMAGING
General Features
• Best diagnostic clue
Bowel wall thickening, mesenteric infiltration, intraperitoneal blood, ± extravasation of enteric or vascular contrast medium
• Location
Duodenum and proximal jejunum are most common sites
Radiographic Findings
• Radiography
Flank stripe sign: Increased density zone separates vertical colon segments from properitoneal fat and peritoneal reflection





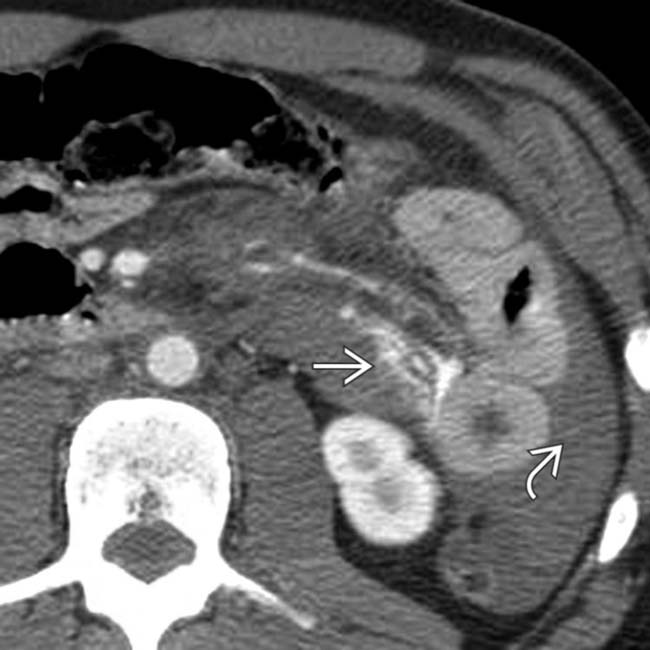
 , adjacent to thick-walled jejunum, and active bleeding, as evidenced by the contrast extravasation
, adjacent to thick-walled jejunum, and active bleeding, as evidenced by the contrast extravasation  . All characteristic findings in intestinal trauma.
. All characteristic findings in intestinal trauma.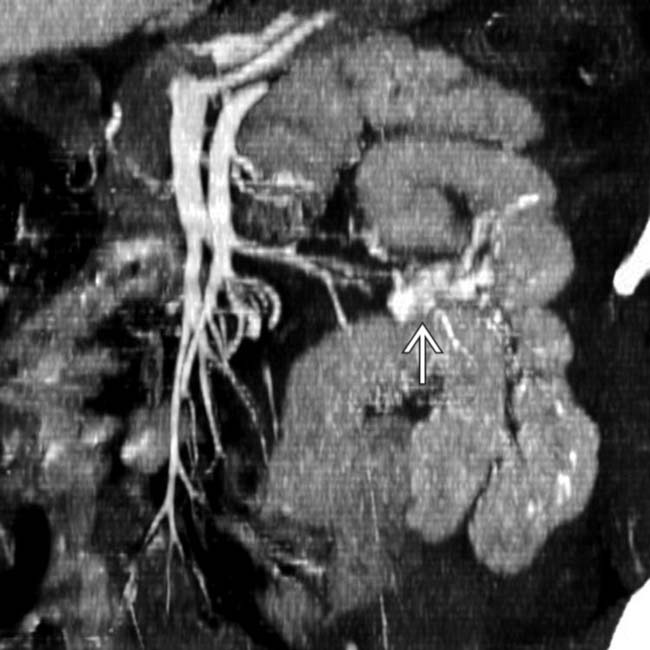
 . The mesenteric injury was surgically repaired and a segment of small intestine was resected.
. The mesenteric injury was surgically repaired and a segment of small intestine was resected.
 adjacent to a thick-walled jejunal segment
adjacent to a thick-walled jejunal segment  , indicative of transmural laceration or perforation.
, indicative of transmural laceration or perforation.
 , a characteristic finding in the setting of intestinal trauma.
, a characteristic finding in the setting of intestinal trauma.




























 Uniform, regular thickening of valvulae conniventes with symmetric, spike-like configuration, decreased luminal diameter simulating “stack of coins”
Uniform, regular thickening of valvulae conniventes with symmetric, spike-like configuration, decreased luminal diameter simulating “stack of coins”







