Most common sites of metastases: Skin, lymph nodes (75%), lung (70%), liver (58%), CNS (54%), GI tract (40%)
Most common sites in abdomen: Liver and small bowel
• Melanoma metastases are often T1 hyperintense on MR due to melanin content
• Lymph nodes
1st nodes to be involved are usually regional lymph nodes with contiguous spread through lymphatic chains
Metastatic nodes may enlarge or change in morphology (↑ enhancement, loss of fatty hilum)
• Liver
Most common site of visceral organ involvement
May be hypervascular on arterial phase and usually hypodense on venous phase
• Gastrointestinal tract
Small bowel most common site (75% of cases)
May present as lead point of small bowel intussusception
Soft tumor that does not usually cause obstruction
• Gallbladder
Melanoma is most common metastasis to gallbladder
• Kidney
Can involve kidney, bladder, or collecting systems
Unique predisposition for perirenal space
Consider melanoma with isolated mass in perirenal space
TOP DIFFERENTIAL DIAGNOSES
• Leukemia and lymphoma
• Metastases from other primary tumors
• Primary GI malignancies
• Kaposi sarcoma
CLINICAL ISSUES
• Risk of metastasis correlates with depth of primary tumor into dermis
(Left) Axial CECT in a patient with known metastatic melanoma demonstrates mass-like wall thickening and aneurysmal dilatation of 2 segments of colon, in keeping with bowel metastases.
(Right) Coronal volume-rendered CECT in the same patient demonstrates 3 different metastases , with several others scattered throughout the small and large bowel (not shown). Lymphoma and GI stromal tumors can also cause similar aneurysmal dilatation.
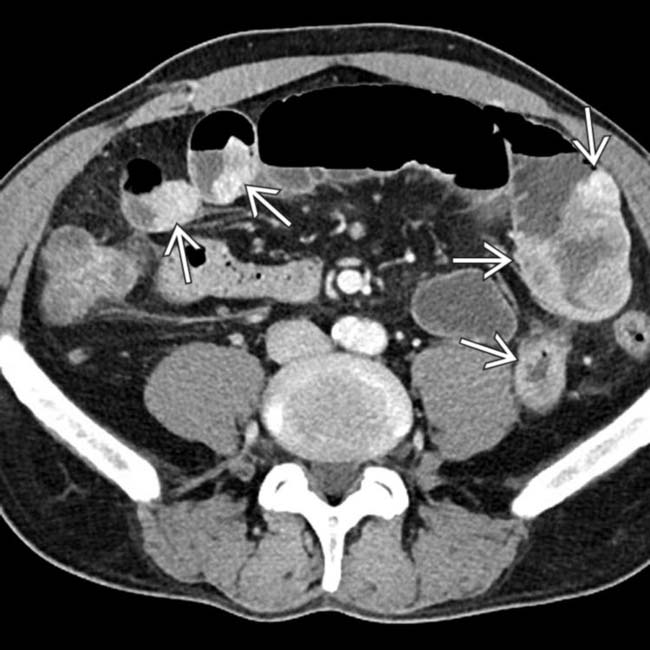
(Left) Axial CECT in a patient with melanoma demonstrates a nodular hypervascular metastasis in the small bowel causing proximal bowel obstruction .
(Right) Axial CECT in the same patient demonstrates multiple other sites of nodular enhancing soft tissue in the small bowel. Multifocal metastases to the bowel are not uncommon in melanoma.
TERMINOLOGY
Definitions
• Spectrum of metastatic lesions originating from known or occult malignant melanoma
IMAGING
General Features
• Best diagnostic clue
Multiple “bull’s-eye” lesions of variable size in GI tract of patient with history of melanoma
• Location
Unique predisposition for metastatic disease to unusual locations (gallbladder, small bowel, spleen, subcutaneous soft tissues, etc.)
– Can metastasize to nearly any location and may have an isolated metastasis in atypical location
– Distant metastases depend on site of primary tumor
Lower extremity melanomas often spread to pelvis
Ocular melanomas frequently spread to liver
Most common sites of metastases: Skin, lymph nodes (75%), lung (70%), liver (58%), CNS (54%), GI tract (40%)
Most common sites in abdomen: Liver and small bowel
• Morphology
Typically multiple, in any site of body
Well-circumscribed, spherical or oval
Nodule, plaque, polypoid mass
“Bull’s-eye” or “target” lesion (central ulceration)
Imaging Recommendations
• Best imaging tool
PET/CT (from vertex through feet) with diagnostic CECT for total body screening
– Sensitivity and specificity are ↑ by simultaneous interpretation of diagnostic quality CT
– Melanoma may not be FDG avid or may be misinterpreted as normal bowel or kidney on PET
• Protocol advice
Multiphase CECT: Melanoma may be hypervascular and metastases may not be visualized on monophasic CECT
Radiographic Findings
• Radiography
Rarely, calcification may be seen in hepatic lesions
CT Findings
• Lymph nodes
First nodes to be involved are usually regional lymph nodes with contiguous spread through lymphatic chains
– Careful assessment necessary of lymph node stations adjacent to primary tumor
– Abdominal nodal involvement in 30% of cases
Metastatic nodes may enlarge or change in morphology (↑ enhancement, loss of fatty hilum, irregular margins)
– Involved lymph nodes may enlarge and bleed
– Rarely necrotic with peripheral enhancement
• Liver
Most common site of visceral organ involvement
– Particularly common with ocular melanoma, and can occur years after initial diagnosis
Single or multiple lesions of variable size ± calcification
– May be hypervascular on arterial phase
– Most (86%) lesions hypodense on portal venous phase
Rim enhancement in lesions with central necrosis
Subcapsular hematoma may result from spontaneous bleeding of hepatic metastases
• Gastrointestinal tract
Can involve any portion of GI tract, but small bowel is most common site (75% of cases)
Can present with a single or multiple lesions, often with central necrosis or ulceration
May lead to aneurysmal dilation of bowel lumen
Predilection for antimesenteric border of small bowel
May present as lead point of small bowel intussusception
Esophagus
– Very rare lesion
– Bulky soft-tissue mass with esophageal dilatation upstream
– More common in distal 1/2
Stomach
– Sessile or pedunculated intraluminal soft-tissue masses ± “target” appearance

 1st nodes to be involved are usually regional lymph nodes with contiguous spread through lymphatic chains
1st nodes to be involved are usually regional lymph nodes with contiguous spread through lymphatic chains










 of 2 segments of colon, in keeping with bowel metastases.
of 2 segments of colon, in keeping with bowel metastases.
 , with several others scattered throughout the small and large bowel (not shown). Lymphoma and GI stromal tumors can also cause similar aneurysmal dilatation.
, with several others scattered throughout the small and large bowel (not shown). Lymphoma and GI stromal tumors can also cause similar aneurysmal dilatation.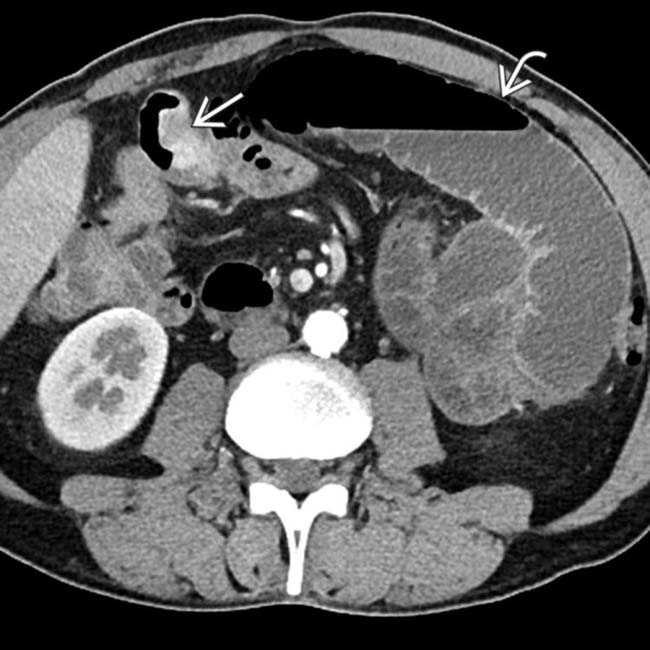
 in the small bowel causing proximal bowel obstruction
in the small bowel causing proximal bowel obstruction  .
.
 in the small bowel. Multifocal metastases to the bowel are not uncommon in melanoma.
in the small bowel. Multifocal metastases to the bowel are not uncommon in melanoma.
 Unique predisposition for metastatic disease to unusual locations (gallbladder, small bowel, spleen, subcutaneous soft tissues, etc.)
Unique predisposition for metastatic disease to unusual locations (gallbladder, small bowel, spleen, subcutaneous soft tissues, etc.)  Most common sites of metastases: Skin, lymph nodes (75%), lung (70%), liver (58%), CNS (54%), GI tract (40%)
Most common sites of metastases: Skin, lymph nodes (75%), lung (70%), liver (58%), CNS (54%), GI tract (40%)









 First nodes to be involved are usually regional lymph nodes with contiguous spread through lymphatic chains
First nodes to be involved are usually regional lymph nodes with contiguous spread through lymphatic chains
















 Single or multiple nodules of variable size with peritoneal/omental stranding, nodularity, and ascites
Single or multiple nodules of variable size with peritoneal/omental stranding, nodularity, and ascites









 Single or multiple lesions of variable size which can appear solid or “cystic” (never simple cystic appearance)
Single or multiple lesions of variable size which can appear solid or “cystic” (never simple cystic appearance)








