Strong tendency to obstruct pancreatic and common bile ducts with abrupt ductal cutoff at site of obstruction
Pancreatic parenchymal atrophy upstream from mass
Soft tissue infiltration to involve adjacent vessels and organs (e.g., duodenum, bowel, stomach, and adrenals)
Most common sites of distant metastatic disease are liver, peritoneum, and lungs
Arterial involvement quantified as < 180° or ≥ 180° tumoral involvement of vessel circumference
Venous involvement may involve abutment, encasement, narrowing, or occlusion
• MR: Tumor conspicuous on T1WI, appearing low signal and juxtaposed against high signal pancreatic parenchyma
T2WI less useful, as tumors isointense to pancreas
Conspicuity on T1WI C+ similar to CT, with tumors demonstrating progressive delayed enhancement
CLINICAL ISSUES
• Most common malignant tumor of exocrine pancreas and accounts for > 95% of pancreatic malignancies
• Most common symptoms are jaundice, weight loss, abdominal pain, and back pain
Often asymptomatic until late in course, particularly body/tail tumors that do not cause jaundice
• Only potentially curative treatment is complete surgical resection with negative surgical margins
• Only 15-20% of patients candidates for surgery at presentation, with 5-year survival of ∼ 20% after surgery
• 5-year survival rate is < 5% without surgery with median survival of 3.5 months
(Left) Graphic shows pancreatic head carcinoma encasing and obstructing the pancreatic and distal bile ducts. There is encasement of the superior mesenteric vessels and spread to celiac nodes . Note the atrophy of the distal body-tail segments .
(Right) Axial CECT in the venous phase demonstrates a poorly marginated hypodense mass in the pancreatic body, typical for pancreatic adenocarcinoma. The mass abuts the distal celiac trunk and the hepatic artery , with < 180° involvement of each.
(Left) Coronal CECT demonstrates a subtle hypodense mass in the pancreatic head resulting in obstruction and upstream dilatation of the pancreatic duct . The presence of pancreatic ductal dilatation and abrupt cut-off should always prompt careful search for a pancreatic mass.
(Right) Sagittal CECT demonstrates a poorly marginated pancreatic cancer encasing the SMA, with 360° involvement. This degree of encasement almost certainly makes this tumor unresectable.
TERMINOLOGY
Synonyms
• Pancreatic adenocarcinoma, pancreatic cancer
Definitions
• Malignancy arising from ductal epithelium of exocrine pancreas
IMAGING
General Features
• Best diagnostic clue
Poorly marginated, hypoenhancing mass with abrupt obstruction of pancreatic duct ± common bile duct
• Location
Head (60%), body (20%), diffuse (15%), tail (5%)
• Size
Variable; average size 2-3 cm
• Morphology
CT Findings
• CT sensitivity for pancreatic cancer is excellent (∼ 97%)
Excellent modality for determining unresectability (positive predictive value for unresectability of 89-100%)
Less effective in determining resectability, as only 60-91% of tumors found to be resectable on CT are actually resectable at surgery
• Poorly marginated, hypodense mass with tendency to infiltrate posteriorly into retroperitoneum
Tumor most conspicuous in portal venous (∼ 70 seconds) and pancreatic (∼ 40 seconds) contrast phases
5% of tumors isodense to pancreas on all phases, requiring attention to secondary signs of tumor
Tumor virtually never calcifies in absence of treatment
• Secondary signs of tumor
Strong tendency to obstruct pancreatic and common bile ducts with abrupt ductal cutoff at site of obstruction
Pancreatic parenchymal atrophy upstream from mass
Abnormal contour of pancreas with loss of normal fatty lobulation and texture
Soft tissue infiltration to involve adjacent vessels and organs (e.g., duodenum, bowel, stomach, and adrenals)
• Distant metastatic disease
Most common sites are liver, peritoneum, and lungs
Regional lymph nodes frequently involved, but CT inaccurate for involvement (sensitivity < 20%)
Adrenals, bones, and pleura (uncommon)
• CT best modality for determining vascular invasion
Arterial involvement quantified as < 180° or ≥ 180° tumoral involvement of vessel circumference
Venous involvement determined based on degree of contact between tumor and vessel, and described as abutment, encasement, narrowing, or occlusion
– Distinction between < 180° or ≥ 180° involvement of veins no longer as important with advent of venous reconstruction
– SMV or splenic vein narrowing often results in mesenteric or gastroepiploic collateral veins
Tumor thrombus in mesenteric veins very uncommon, and much more common with neuroendocrine tumors
• Pancreatic adenocarcinoma classically causes hypercoagulability: Look for evidence of incidental pulmonary emboli or deep venous thrombosis
MR Findings
• Normal pancreas
Diffusely high signal intensity on T1WI (≥ liver)
Parenchyma variable in signal on T2WI
Pancreas enhances avidly and homogeneously on T1WI C+ (hyperintense to liver on arterial phase and isointense on delayed phase)
• MR particularly helpful in identifying small group of tumors that are isodense to normal pancreas on CT
• Tumor conspicuous on T1WI, appearing low signal and juxtaposed against high signal pancreatic parenchyma
Atrophic pancreas upstream from tumor often abnormally low signal on T1WI
• T2WI generally not useful for tumor detection, as tumors often isointense to pancreas
• Conspicuity on T1WI C+ similar to CT, with hypovascular tumors often demonstrating progressive delayed enhancement
• Tumors often demonstrate restricted diffusion with lower ADC values than adjacent normal pancreas
DWI not helpful in differentiating tumors from other entities (such as autoimmune pancreatitis)
• MRCP and T2WI can nicely demonstrate abrupt cutoff and obstruction of pancreatic and common bile ducts
• MR generally 2nd choice (behind CT) for evaluating vascular involvement
Ultrasonographic Findings
• Hypoechoic mass with only minimal internal color Doppler flow vascularity
• Biliary dilatation and pancreatic ductal dilatation upstream from tumor
• Endoscopic ultrasound: Similar to conventional US findings, with inferior accuracy compared to CECT for locoregional staging or determining vascular involvement
Helpful in excluding malignancy in patients with indeterminate CT findings (↑ negative predictive value)
Can help guide biopsy of pancreatic masses
Nuclear Medicine Findings
• PET/CT
PET alone (without diagnostic CT) not effective for diagnosis of primary tumor (sensitivity as low as 72%)
– Possible role in differentiating malignant from benign lesions, as FDG-avid lesions have ↑ risk of malignancy
May help differentiate pancreatic adenocarcinoma, which shows avid focal uptake in mass, from focal autoimmune pancreatitis, which shows diffuse uptake throughout pancreas and within salivary glands
– Effective in judging response to treatment (chemoradiation), whereas CT may not differentiate post-treatment fibrosis from residual tumor
PET not helpful for vascular involvement or locoregional staging (e.g., lymph nodes) due to poor spatial resolution
Helpful for distant staging, and may change resectability status of ∼ 20% of patients compared to CECT
Radiographic Findings
• Barium (upper GI) study
Frostberg 3 sign: “Inverted 3” contour to medial part of duodenal sweep
Spiculated duodenal wall with traction, fixation, and widening of duodenal sweep
Antral padding: Extrinsic indentation by tumor of posteroinferior margin of antrum
• ERCP
Irregular, abrupt, nodular, rat-tailed, eccentric obstruction of pancreatic and common bile ducts
Double duct sign: Obstruction of pancreatic and common bile duct at same level
Localized encasement with prestenotic dilatation
Angiographic Findings
•
Imaging Recommendations
• Best imaging tool
Dual-phase CECT with arterial and portal venous phases
• Protocol advice
Best phase for identifying pancreatic cancers is pancreatic phase at ∼ 40 seconds after contrast
Portal venous phase nearly equivalent for tumor detection and allows optimal evaluation of liver metastases and central mesenteric veins
Arterial phase critical for evaluating relationship of tumor to mesenteric arteries
Most institutions no longer acquire 3 phases, as arterial and portal venous phases are sufficient
Multiplanar views improve detection and depiction of ductal obstruction, vascular encasement, nodes
• CT and MR
High predictive value (near 100%) for tumor nonresectability
Less predictive value (75-85%) for resectable tumor
• Endoscopic US
Excellent for detection and staging of small tumor
Facilitates biopsy for tissue confirmation
DIFFERENTIAL DIAGNOSIS
Pancreatic Neuroendocrine Tumors
• Well-circumscribed mass that is typically markedly hypervascular on arterial phase images
• Usually no ductal obstruction or parenchymal atrophy
• Frequently calcify and may invade mesenteric veins with tumor thrombus (unusual features for pancreatic adenocarcinoma)
Focal Autoimmune Pancreatitis
• Classic appearance is sausage-like diffuse enlargement of pancreas with peripheral peripancreatic “halo”
• Can rarely manifest as focal hypodense pancreatic mass that may appear identical to adenocarcinoma
• Upstream pancreas usually enlarged, rather than atrophic, and pancreatic duct usually not dilated
• Typically responds dramatically to steroid therapy
Chronic Pancreatitis
• May be associated with focal fibroinflammatory mass that can be indistinguishable from pancreatic cancer
• Usually other stigmata of chronic pancreatitis, including diffuse atrophy of gland, dilated/beaded pancreatic duct with ductal calculi, and parenchymal calcifications
• May obstruct both pancreatic and common bile ducts, producing double duct sign (similar to adenocarcinoma)
• Given that chronic pancreatitis is a major risk factor, chronic pancreatitis and pancreatic adenocarcinoma may coexist
Pancreatic Metastases and Lymphoma
• Hypovascular metastases (e.g., lung, colon) to pancreas may mimic pancreatic adenocarcinoma, but typically evidence of widespread metastatic disease elsewhere
Less commonly obstruct pancreatic duct or CBD
• Lymphoma presents as homogeneous, hypoenhancing soft tissue mass
Almost never causes ductal obstruction/dilatation or parenchymal atrophy
Usually occurs in setting of disseminated disease, with significant surrounding lymphadenopathy
Encases peripancreatic vessels without narrowing or occlusion
Asymmetric Fatty Infiltration of Pancreatic Head
• May superficially mimic tumor, but no mass effect, ductal dilatation, or other secondary signs of malignancy
• MR with in- and out-of-phase imaging can easily make distinction between fatty infiltration and tumor
Mucinous Cystic Pancreatic Tumor
• Cystic component may not be recognized on NECT
• Usually does not obstruct pancreatic or bile duct
Tumors From Adjacent Organs
• Duodenal adenocarcinoma or GI stromal tumors (GIST) involving distal stomach or duodenum may be difficult to distinguish from primary pancreatic mass
Groove Pancreatitis
• Form of chronic pancreatitis affecting pancreaticoduodenal groove
Only gold members can continue reading. Log In or Register to continue

 Soft tissue infiltration to involve adjacent vessels and organs (e.g., duodenum, bowel, stomach, and adrenals)
Soft tissue infiltration to involve adjacent vessels and organs (e.g., duodenum, bowel, stomach, and adrenals)





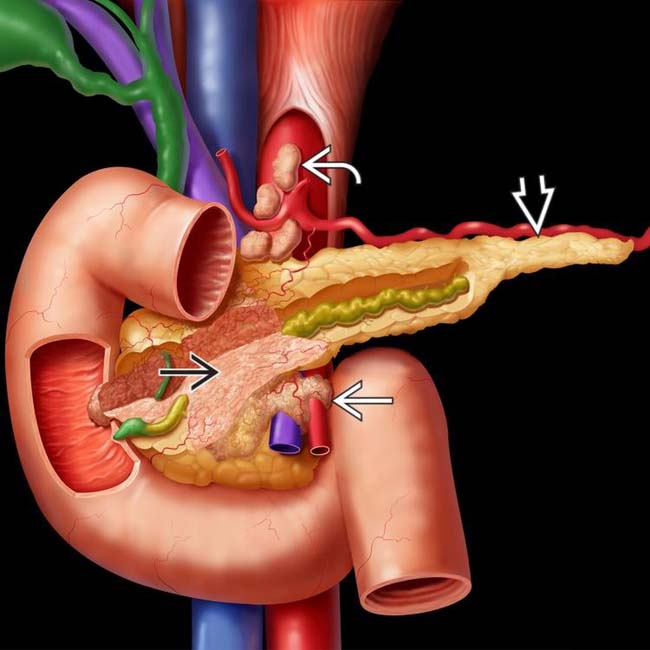
 encasing and obstructing the pancreatic and distal bile ducts. There is encasement of the superior mesenteric vessels
encasing and obstructing the pancreatic and distal bile ducts. There is encasement of the superior mesenteric vessels  and spread to celiac nodes
and spread to celiac nodes  . Note the atrophy of the distal body-tail segments
. Note the atrophy of the distal body-tail segments  .
.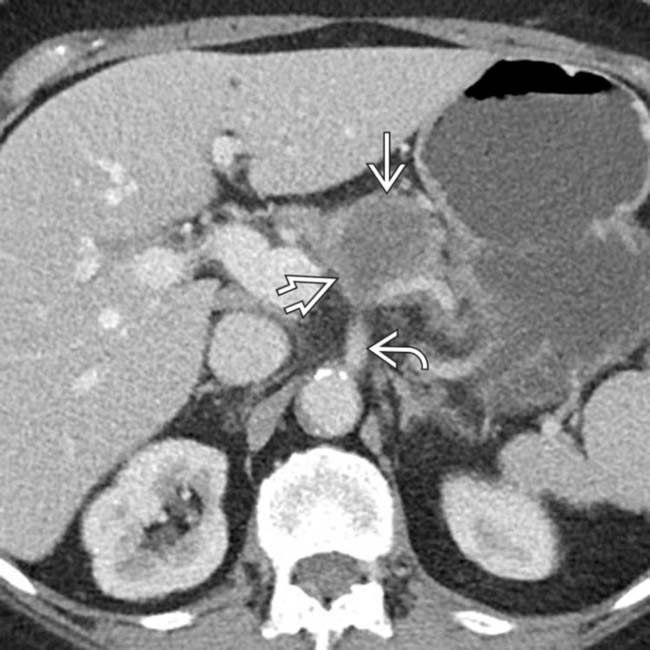
 in the pancreatic body, typical for pancreatic adenocarcinoma. The mass abuts the distal celiac trunk
in the pancreatic body, typical for pancreatic adenocarcinoma. The mass abuts the distal celiac trunk  and the hepatic artery
and the hepatic artery  , with < 180° involvement of each.
, with < 180° involvement of each.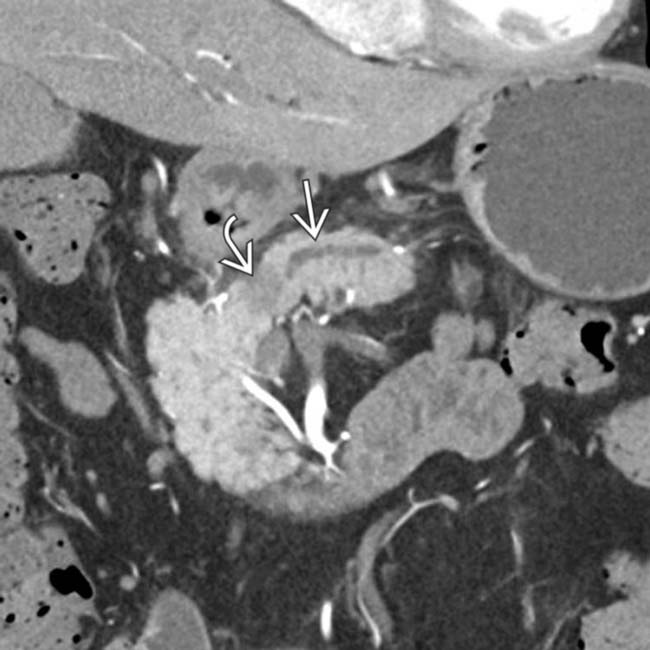
 in the pancreatic head resulting in obstruction and upstream dilatation of the pancreatic duct
in the pancreatic head resulting in obstruction and upstream dilatation of the pancreatic duct  . The presence of pancreatic ductal dilatation and abrupt cut-off should always prompt careful search for a pancreatic mass.
. The presence of pancreatic ductal dilatation and abrupt cut-off should always prompt careful search for a pancreatic mass.
 encasing the SMA, with 360° involvement. This degree of encasement almost certainly makes this tumor unresectable.
encasing the SMA, with 360° involvement. This degree of encasement almost certainly makes this tumor unresectable.



 Excellent modality for determining unresectability (positive predictive value for unresectability of 89-100%)
Excellent modality for determining unresectability (positive predictive value for unresectability of 89-100%)
 Tumor most conspicuous in portal venous (∼ 70 seconds) and pancreatic (∼ 40 seconds) contrast phases
Tumor most conspicuous in portal venous (∼ 70 seconds) and pancreatic (∼ 40 seconds) contrast phases

 Strong tendency to obstruct pancreatic and common bile ducts with abrupt ductal cutoff at site of obstruction
Strong tendency to obstruct pancreatic and common bile ducts with abrupt ductal cutoff at site of obstruction





 Venous involvement determined based on degree of contact between tumor and vessel, and described as abutment, encasement, narrowing, or occlusion
Venous involvement determined based on degree of contact between tumor and vessel, and described as abutment, encasement, narrowing, or occlusion








 PET alone (without diagnostic CT) not effective for diagnosis of primary tumor (sensitivity as low as 72%)
PET alone (without diagnostic CT) not effective for diagnosis of primary tumor (sensitivity as low as 72%) PET not helpful for vascular involvement or locoregional staging (e.g., lymph nodes) due to poor spatial resolution
PET not helpful for vascular involvement or locoregional staging (e.g., lymph nodes) due to poor spatial resolution


























