Well-defined cystic lesion with variable morphology: Unilocular, multicystic, or tubular
Communication with adjacent main pancreatic duct is key to diagnosis (may be more visible on MR than CT)
Dilatation of adjacent main pancreatic duct should raise concern for main duct involvement
Multiplicity is strong clue to diagnosis: Often multiple small cysts scattered throughout pancreas
• Main duct IPMN
Markedly dilated, tortuous MPD often with bulging ampulla filled with fluid (mucin)
Dilatation may be segmental or diffuse
Polypoid nodularity in MPD suspicious for malignancy
Amorphous calcifications may be seen within duct
Pancreas often atrophic overlying dilated duct
• Combined IPMN
Cystic lesion in contiguity with dilated MPD (shares imaging features of main duct and side branch IPMN)
CLINICAL ISSUES
• EUS cyst aspiration: Elevated cyst fluid CEA (> 192 ng/mL)
• Most patients asymptomatic (incidental imaging finding), but can result in repetitive bouts of pancreatitis
• Risk of transformation into invasive carcinoma, with main duct involvement associated with ↑ risk of malignancy
• Management of IPMN based on 2012 IAP guidelines
Worrisome features: Cyst size ≥ 3 cm, MPD dilatation 5-9 mm, peripheral wall thickening, nonenhancing mural nodularity, abrupt change in main duct caliber with upstream pancreatic atrophy
High-risk features: MPD dilatation ≥ 1 cm, enhancing solid mural nodularity, or biliary obstruction
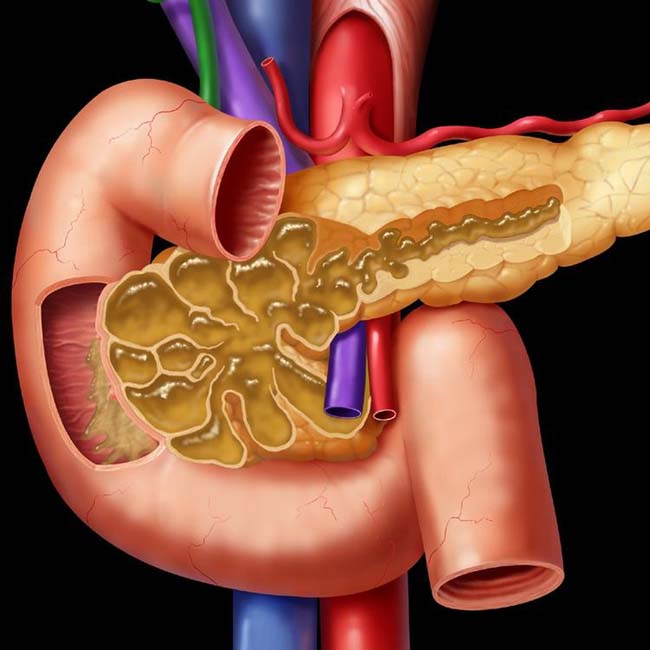
(Left) Graphic shows combined main and side branch IPMN with gross dilatation of all ducts by mucin, which pours out of a bulging papilla into the duodenum. The parenchyma in the pancreatic head is atrophic.
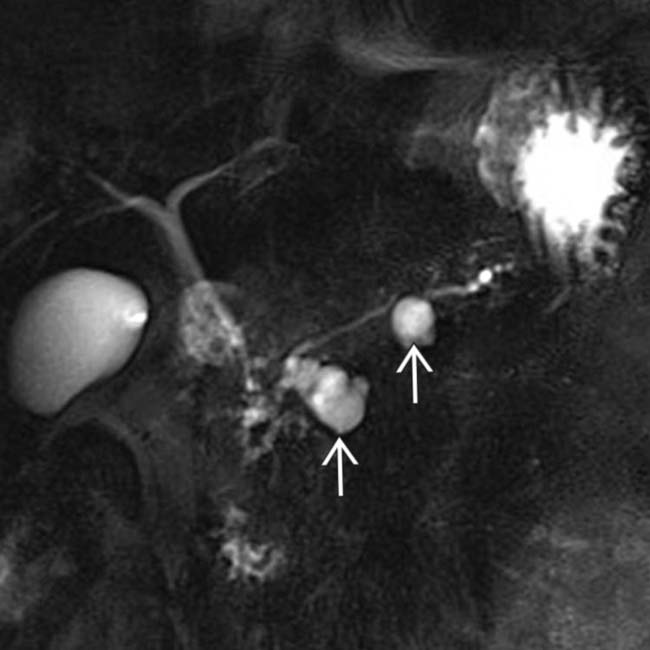
(Right) Coronal MRCP with MIP reconstruction nicely demonstrates 2 discrete side branch IPMNs and their direct connection with the adjacent normal sized pancreatic duct.
(Left) Coronal MRCP with MIP reconstruction demonstrates multiple cysts throughout the pancreas compatible with multiple side branch IPMN. Multifocality is characteristic of IPMN, and multiple discrete cystic lesions are often present in the same patient.
(Right) Coronal CECT demonstrates innumerable pancreatic cysts, compatible with multiple side branch IPMN. No suspicious individual cyst or solid mass was seen, but EUS findings were suspicious, and the patient was found to have invasive carcinoma at surgery.
• Mucin-producing papillary tumor arising from epithelium of main pancreatic duct (MPD) or pancreatic duct side branches
IMAGING
General Features
• Best diagnostic clue
Side branch type: Cystic lesion with direct communication with adjacent MPD on CECT/MRCP
MPD type: Dilated MPD with bulging papilla and enhancing soft tissue nodularity within duct lumen
• Location
Side branch lesion: Predisposition for uncinate process and head, but can occur anywhere in pancreas
MPD lesion: Either diffuse or segmental involvement of pancreatic duct, but most often involves body and tail
• Size
Side branch cysts: Variable, but most side branch IPMN measure 5-20 mm
• Morphology
IPMN: Subdivision of mucin-producing tumors (along with mucinous cystic neoplasm)
Classified into 3 types
– Side branch pancreatic duct (BPD) type: Focal lobulated “multicystic” dilatation of branch ducts
– Main pancreatic duct (MPD) type: Diffuse dilatation of main pancreatic duct
– Combined type: Dilatation of both BPD and MPD
CT Findings
• Side branch IPMN
Well-defined cystic lesion with variable morphology: Unilocular, multicystic (with grape-like clusters or tubes and arcs), or tubular
Communication with adjacent MPD is key to diagnosis, but may not always be possible to demonstrate
– May be more apparent on multiplanar reformations
– Dilatation of adjacent main pancreatic duct should raise concern for main duct involvement
Multiplicity is strong clue to diagnosis: Often multiple small cysts scattered throughout pancreas
Calcifications in 20%, but no correlation with malignancy
• Main duct IPMN
Markedly dilated, tortuous MPD without evidence of distal obstructing mass and often with “bulging” ampulla filled with fluid (mucin) at duodenal sweep
– Dilatation may be segmental or diffuse
– Possibility of main duct IPMN should be considered when duct measures ≥ 5 mm
Presence of polypoid enhancing nodularity within MPD lumen is very suspicious for malignancy
Amorphous calcifications may be seen within duct
Pancreas often atrophic overlying dilated duct
• Combined IPMN
Cystic lesion in contiguity with dilated MPD (shares imaging features of main duct and side branch IPMN)
• Concerning imaging features based on 2012 International Association of Pancreatology (IAP) guidelines
Worrisome features: Cyst size ≥ 3 cm in any dimension, MPD dilatation between 5-9 mm, peripheral wall thickening or enhancement, nonenhancing mural nodularity, abrupt change in main duct caliber with distal pancreatic atrophy, lymphadenopathy
High-risk features: MPD dilatation ≥ 1 cm, enhancing solid mural nodularity, or biliary obstruction
MR Findings
• Little data directly comparing CT and MR, but MR likely superior for identifying small cysts and multifocal disease, visualizing communication between cyst and main duct, and assessing main duct involvement
Superior soft tissue resolution of MR may allow better assessment of subtle mural nodularity
• Side branch IPMN typically hyperintense on T2WI and low signal on T1WI, and can appear unilocular, multicystic, tubular, or as grape-like cluster of cysts
Presence of dilated adjacent main pancreatic duct concerning for main duct involvement
– MRCP may be more accurate than CT for assessing main duct size and internal mural nodularity
• Direct communication with main pancreatic duct easier to identify on thin-section 3D MRCP images
Enlargement of cyst following administration of secretin may be secondary sign of communication with main duct
• Malignant IPMN may have lower ADC values on DWI compared to benign IPMN, but not widely clinically utilized (due to overlap in ADC values)
Ultrasonographic Findings
• Conventional ultrasound lacks spatial resolution to identify high-risk or worrisome imaging features
• Endoscopic ultrasound (EUS): Now considered important part of evaluation of pancreatic cysts in specialized centers
Spatial resolution of EUS may help identify suspicious morphologic features (e.g., mural nodularity) not visible on CT/MR, and can help guide FNA and cyst aspiration
– May identify communication between cyst and MPD
2012 IAP guidelines recommend EUS with cyst aspiration for cysts with worrisome imaging features
– Cyst size ≥ 3 cm, MPD dilatation 5-9 mm, peripheral wall thickening, nonenhancing mural nodularity, etc.
Radiographic Findings
• ERCP
Direct visualization of patulous, bulging, “fish-mouth” ampulla with mucin extruding through ampulla (due to mucin hypersection) in main duct IPMN
Can directly demonstrate dilatation of MPD (in main duct IPMN) or communication of side branch IPMN with MPD
Filling defects within duct (either nodular or band-like) may represent mucin or papillary tumors
Imaging Recommendations
• Best imaging tool
MR or CECT are best initial noninvasive modalities
EUS utilized for lesions with suspicious imaging features
DIFFERENTIAL DIAGNOSIS
Chronic Pancreatitis
• Dilated, beaded, irregular main pancreatic duct with intraductal calculi and parenchymal atrophy/calcifications
• Significant imaging/clinical overlap with main duct IPMN
Pancreatic Ductal Carcinoma
• Hypodense mass with abrupt cutoff of pancreatic duct and upstream MPD dilatation/parenchymal atrophy
• Small occult lesion obstructing MPD may appear identical to main duct IPMN
Pancreatic Pseudocyst
• Cystic lesions that may communicate with MPD and can mimic side branch IPMN
• Usually known clinical history of pancreatitis (or risk factors) and inflammatory changes surrounding cyst
Mucinous Cystic Pancreatic Tumor
• Cyst (± thick wall) most often occurring in pancreatic body/tail in middle-aged female
Only gold members can continue reading. Log In or Register to continue
 Communication with adjacent main pancreatic duct is key to diagnosis (may be more visible on MR than CT)
Communication with adjacent main pancreatic duct is key to diagnosis (may be more visible on MR than CT)









 and their direct connection with the adjacent normal sized pancreatic duct.
and their direct connection with the adjacent normal sized pancreatic duct.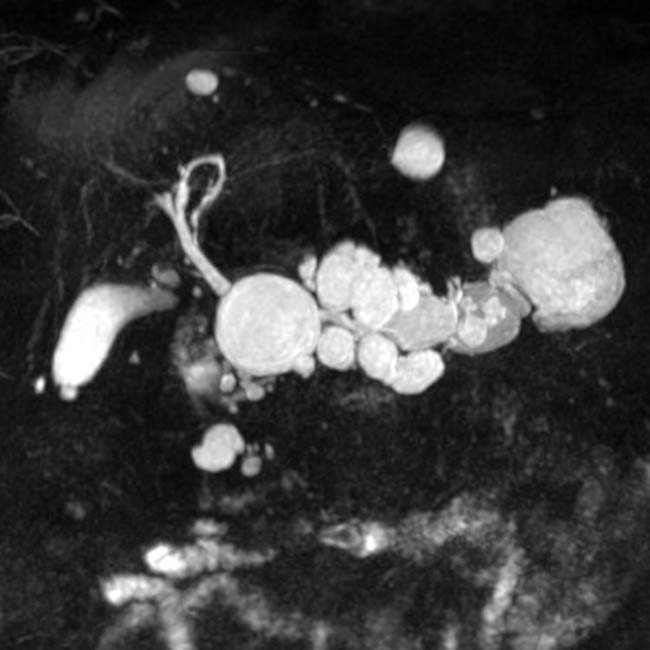



 Side branch lesion: Predisposition for uncinate process and head, but can occur anywhere in pancreas
Side branch lesion: Predisposition for uncinate process and head, but can occur anywhere in pancreas



 Well-defined cystic lesion with variable morphology: Unilocular, multicystic (with grape-like clusters or tubes and arcs), or tubular
Well-defined cystic lesion with variable morphology: Unilocular, multicystic (with grape-like clusters or tubes and arcs), or tubular


 Markedly dilated, tortuous MPD without evidence of distal obstructing mass and often with “bulging” ampulla filled with fluid (mucin) at duodenal sweep
Markedly dilated, tortuous MPD without evidence of distal obstructing mass and often with “bulging” ampulla filled with fluid (mucin) at duodenal sweep



 Worrisome features: Cyst size ≥ 3 cm in any dimension, MPD dilatation between 5-9 mm, peripheral wall thickening or enhancement, nonenhancing mural nodularity, abrupt change in main duct caliber with distal pancreatic atrophy, lymphadenopathy
Worrisome features: Cyst size ≥ 3 cm in any dimension, MPD dilatation between 5-9 mm, peripheral wall thickening or enhancement, nonenhancing mural nodularity, abrupt change in main duct caliber with distal pancreatic atrophy, lymphadenopathy















