Secondary signs of pancreatic injury are usually present (peripancreatic fat stranding and fluid, thickening of pararenal fascia, peripancreatic hematoma)
– Peripancreatic signs of traumatic pancreatitis often subtle; more evident in 24-48 hours
Pancreatic contusion: Ill-defined focal hypoattenuation at site of injury (not linear like laceration)
Pancreatic laceration: Discrete linear hypodense cleft through pancreas
Pancreatic fracture: Large laceration with clear separation of 2 ends of gland
CT insensitive for pancreatic duct injury (usually inferred by laceration extending through duct)
• MR: MRCP (± secretin) is a useful tool in determining presence of pancreatic ductal disruption
• ERCP: Best modality for pancreatic ductal injury
Transection of pancreatic duct: Abrupt duct termination or contrast extravasation
PATHOLOGY
• May result from either penetrating or blunt trauma
Blunt traumatic injury usually results from anterior/posterior compression force to abdomen
• Pancreatic injuries almost never isolated and usually associated with polytrauma
CLINICAL ISSUES
• Blunt pancreatic injuries often clinically occult and unrecognized on initial evaluation
• Clinical presentation often due to traumatic pancreatitis: Upper abdominal pain, abdominal distention
• Serum amylase/lipase levels: Elevated in 90% of patients, but may be normal immediately after trauma
• Treatment: Penetrating trauma generally requires immediate laparotomy
AAST grades I and II: Conservative management
AAST grades III, IV, and V: Typically require surgery (including possible pancreatic resection)
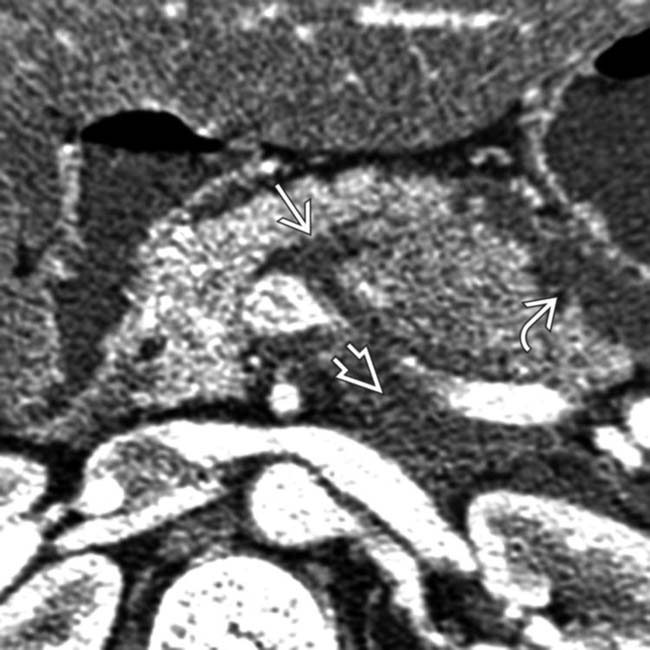
(Left) Axial CECT shows subtle laceration of the pancreas with fluid in the lesser sac as well as retropancreatic fluid .
(Right) Axial CECT in the same patient reveals fluid tracking posterior to the pancreas along the splenic vein from extravasated pancreatic juice. Secondary signs of injury, such as peripancreatic fluid, hematoma, or fat stranding, are almost always present as a clue to the diagnosis.
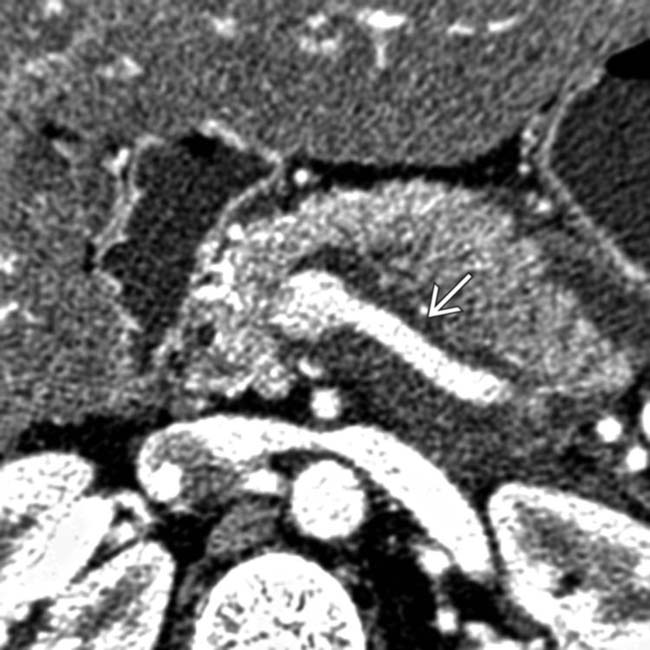
(Left) Axial CECT in a patient with pancreatic fracture shows a fracture plane through the neck of the pancreas. The pancreatic duct was disrupted, and the body and tail of the pancreas were resected at surgery.
(Right) Axial CECT 48 hours after trauma shows a pseudocyst in the lesser sac in this pancreatic transection .The fluid collection developed as a result of leakage of fluid from the site of the transected pancreatic duct.
TERMINOLOGY
Synonyms
• Traumatic pancreatic injury
Definitions
• Inflammatory disease of pancreas secondary to trauma
IMAGING
General Features
• Best diagnostic clue
Enlarged, heterogeneous pancreas with peripancreatic fluid or hematoma in patient with history of trauma
• Location
Most commonly involves pancreatic body > head > tail
• Morphology
Spectrum of injury: Acute pancreatitis, contusions, deep lacerations, fractures with ductal disruption
Radiographic Findings
• ERCP
Normal in cases of pancreatic contusion
Best modality to identify pancreatic duct (PD) injury
– Transection of PD: Abrupt duct termination or contrast extravasation
– Communication of pseudocyst with PD
May cause pancreatitis
CT Findings
• Secondary signs of pancreatic injury or post-traumatic pancreatitis usually present even in absence of discrete contusion/laceration
Peripancreatic fat stranding and fluid with loss of normal peripancreatic fat planes almost always present
– Fluid separating pancreas from splenic vein is sensitive (60-90%) for pancreatic injury
– Fluid or hematoma is often seen in lesser sac, left anterior pararenal space, transverse mesocolon, adjacent to spleen, and mesenteric root
Thickening of anterior pararenal fascia
Peripancreatic or intrapancreatic hematoma: Intrapancreatic hematoma is more specific for pancreatic injury
Peripancreatic signs of traumatic pancreatitis are often subtle: May be more evident in 24-48 hours
• Pancreatic contusion: Ill-defined focal hypoattenuation at site of injury
Appearance ranges from subtle contour deformity of pancreas to rounded mass-like enlargement of pancreas several cm in diameter
Often associated with focal or diffuse pancreatic enlargement
• Pancreatic laceration: Discrete linear cleft of hypoattenuation running through pancreas (usually perpendicular to long-axis of gland)
Much more likely to be associated with PD injuries than contusion
Often associated with distortion or irregularity of contour of pancreas and hypoenhancement of gland upstream from laceration
Lacerations may produce subtle parenchymal density changes and may be undetectable on CT in some cases
– 20-40% of pancreatic injuries not visible on initial imaging
– May only be faintly visible on initial imaging, and become more conspicuous on follow-up imaging
CT is not sensitive for detection of PD injury (∼ 40%): Inferred by presence of laceration extending through duct (> 50% of pancreatic thickness)
• Pancreatic fracture: Linear low attenuation running through pancreatic parenchyma with clear separation of 2 ends of gland
Most often through pancreatic neck
• Pancreatitis secondary to ERCP (± papillotomy, etc.) usually more severe in/around pancreatic head
MR Findings
• Variably decreased signal on T1WI at sites of contusion or laceration ± high T1 signal related to hematoma
• High signal on T2WI at sites of contusion or laceration
• Heterogeneous enhancement on T1WI C+ images with areas of nonenhancement related to fluid collections, pseudocysts, necrosis, laceration, or severe contusion
• MRCP useful tool to determine PD disruption
Secretin stimulation may improve diagnostic sensitivity
Ductal injury suggested by discontinuity in PD, along with direct communication to adjacent pseudocyst or fluid collection
Ultrasonographic Findings
• Not sensitive for pancreatic injury or complications
• Findings similar to pancreatitis (enlarged, hypoechoic gland)
Imaging Recommendations
• Best imaging tool
CECT for initial evaluation after trauma
Emergency ERCP: Investigate pancreatic injuries when CT positive and status of PD uncertain
• Protocol advice
• Repeat CT at 24-48 hours may identify pancreatic injuries not appreciated on original examination
DIFFERENTIAL DIAGNOSIS
Shock Pancreas
• Part of hypoperfusion complex seen in severe traumatic injuries or in setting of severe hypotension
• Abnormally intense enhancement of pancreas, bowel wall, and kidneys, with decreased caliber of aorta and inferior vena cava, and diffuse dilatation of intestine with fluid
Findings resolve spontaneously after fluid resuscitation
• Moderate to large peritoneal fluid collections
• Pancreas appears edematous, enlarged, and hyperenhancing with surrounding fluid and fat stranding, mimicking post-traumatic pancreatitis or injury
• Differentiate from direct traumatic injury by looking for other imaging features of hypoperfusion complex
Duodenal Injury Without Pancreatic Injury
• Duodenal injury (including rupture or hematoma) may simulate or coexist with pancreatic injury
• Duodenal hematoma appears as focal high-attenuation thickening of duodenal wall
Picket-fence appearance on fluoroscopy from hemorrhage
Smooth intramural mass causing incomplete bowel obstruction
Only gold members can continue reading. Log In or Register to continue
 Pancreatic contusion: Ill-defined focal hypoattenuation at site of injury (not linear like laceration)
Pancreatic contusion: Ill-defined focal hypoattenuation at site of injury (not linear like laceration)






 with fluid in the lesser sac
with fluid in the lesser sac  as well as retropancreatic fluid
as well as retropancreatic fluid  .
.
 tracking posterior to the pancreas along the splenic vein from extravasated pancreatic juice. Secondary signs of injury, such as peripancreatic fluid, hematoma, or fat stranding, are almost always present as a clue to the diagnosis.
tracking posterior to the pancreas along the splenic vein from extravasated pancreatic juice. Secondary signs of injury, such as peripancreatic fluid, hematoma, or fat stranding, are almost always present as a clue to the diagnosis.
 through the neck of the pancreas. The pancreatic duct was disrupted, and the body and tail of the pancreas were resected at surgery.
through the neck of the pancreas. The pancreatic duct was disrupted, and the body and tail of the pancreas were resected at surgery.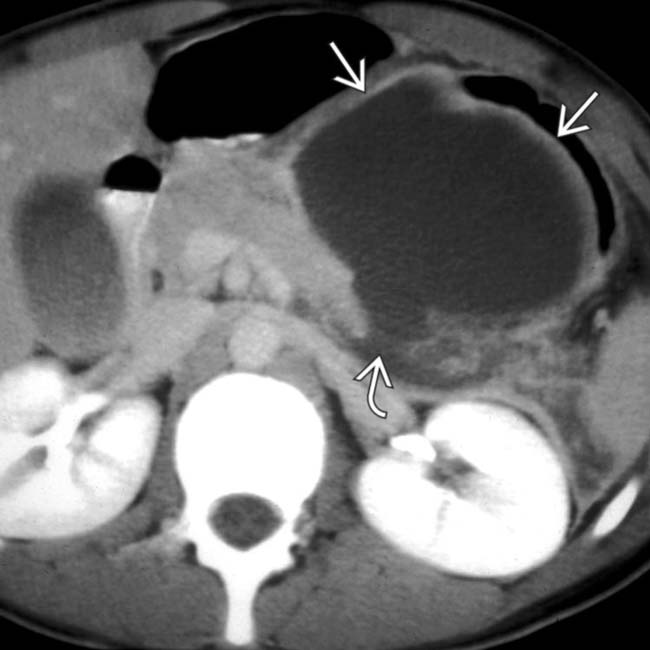
 in the lesser sac in this pancreatic transection
in the lesser sac in this pancreatic transection  .The fluid collection developed as a result of leakage of fluid from the site of the transected pancreatic duct.
.The fluid collection developed as a result of leakage of fluid from the site of the transected pancreatic duct.





 Peripancreatic fat stranding and fluid with loss of normal peripancreatic fat planes almost always present
Peripancreatic fat stranding and fluid with loss of normal peripancreatic fat planes almost always present Peripancreatic or intrapancreatic hematoma: Intrapancreatic hematoma is more specific for pancreatic injury
Peripancreatic or intrapancreatic hematoma: Intrapancreatic hematoma is more specific for pancreatic injury

 Appearance ranges from subtle contour deformity of pancreas to rounded mass-like enlargement of pancreas several cm in diameter
Appearance ranges from subtle contour deformity of pancreas to rounded mass-like enlargement of pancreas several cm in diameter
 Often associated with distortion or irregularity of contour of pancreas and hypoenhancement of gland upstream from laceration
Often associated with distortion or irregularity of contour of pancreas and hypoenhancement of gland upstream from laceration Lacerations may produce subtle parenchymal density changes and may be undetectable on CT in some cases
Lacerations may produce subtle parenchymal density changes and may be undetectable on CT in some cases 
















