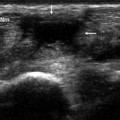
Fig. 12.1
The five annular pulleys (a) are located at the levels of the metacarpophalangeal joint (A1), the proximal phalanx (A2), the proximal interphalangeal joint (A3), the middle phalanx (A4), and the distal interphalangeal joint (A5) of each finger. Their function is to stabilize the flexor tendons. On ultrasound imaging (b), the pulleys are depicted as hypoechogenic (due to anisotropy), ribbon-like structures (arrows) that encircle the flexor digitorum superficialis and profundus tendons (Fle di) and stabilize them on the underlying bone plane
The annular pulleys can be damaged by repeated microtrauma or acute trauma. The result is the condition known as ‘trigger finger’ [1, 3] (Figs. 12.2, 12.3), the pathogenesis of which is the same as that of de Quervain’s disease, namely a loss of equilibrium between the flexor digitorum tendons and the A1 pulley. On ultrasound imaging, the pulley appears thickened, and the acute phases are characterized by flexor tendon tenosynovitis with anechoic fluid within the tendon sheath.
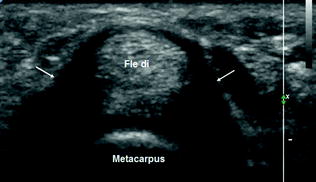
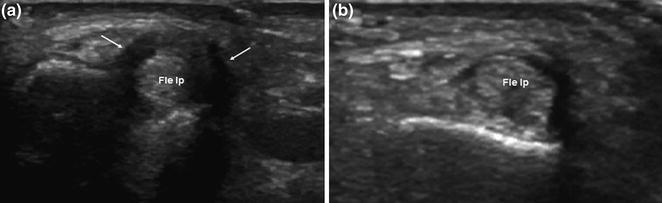
Fig. 12.2
Trigger finger: Sonographic imaging reveals marked thickening and hypoechogenicity (arrows) of the A1 pulley, which surrounds the flexor digitorum superficialis and profundus tendons (Fle di)
Fig. 12.3
Trigger finger: This sonogram depicts the A1 pulley surrounding the flexor pollicis longus tendon (Fle lp). The pulley is markedly thickened and hypoechogenic (arrows) (a); concomitant tenosynovitis of the flexor pollicis longus (b)
Acute tears of the annular pulleys are typically seen in rock climbers [1, 4], and they usually involve the middle finger and/or the ring finger.
Acute injuries unrelated to sport activities are much less common. They all occur when the finger is extended against resistance. The sonographic examination (Figs. 12.4, 12.5) reveals variable anterior subluxation of the two flexor tendons, which are no longer in contact with the bone plane. In the acute phase, there is usually a bloody effusion (hypoechoic/anechoic) in the tendon sheath, between the tendon and the underlying bones. When the finger is flexed against resistance, the anterior instability increases. The injured pulley can rarely be visualized on ultrasound.
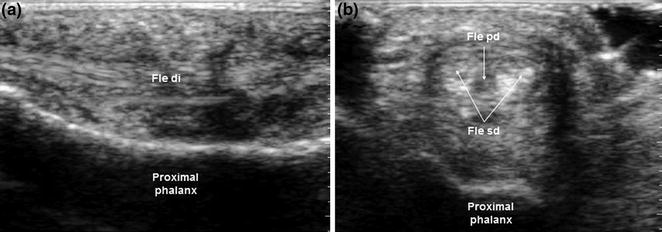
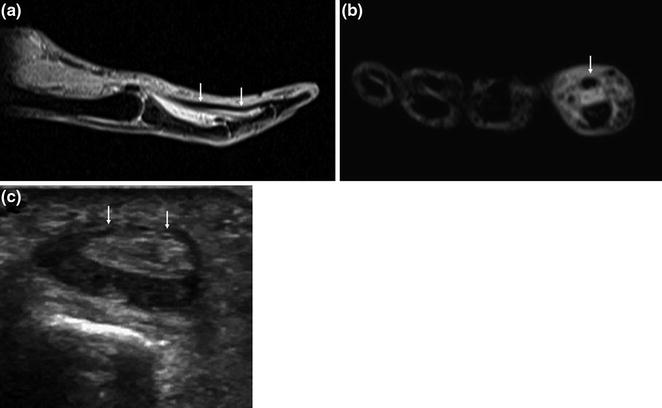
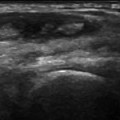
Fig. 12.4
Rock climber’s finger: Acute traumatic rupture of the annular pulleys. The sonogram shows anterior subluxation of the two flexor digitorum tendons (Fle di) and distance between the tendons and the underlying bones. In the acute phase, a hypoechoic/anechoic, bloody effusion is typically observed in the tendon sheath, between the tendons and underlying bone (a, b)
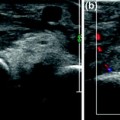
Fig. 12.5
Traumatic rupture of the A2 pulley. MRI (a sagittal scan; b axial scan) and ultrasound imaging (c) reveal anterior subluxation of the two flexor tendons (arrows), which are no longer in contact with the bone plane, and effusion inside the tendon sheath, between the tendons and underlying bone
Ganglia are the most common space-occupying lesions of the wrist and hand [1, 5




Related posts:



Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
