Air-fluid levels on upright or decubitus radiograph
• Transition zone between dilated and collapsed bowel is critical to define presence, site, and cause of obstruction
All better determined on CT than on plain films (accuracy near 100% for high-grade SBO)
• Small bowel feces sign: Gas bubbles mixed with particulate matter in dilated loops just proximal to site of obstruction
• “Positive” oral contrast medium for CT is rarely useful
• Closed loop obstruction
SB segments are markedly distended (> 4 cm) by fluid, little gas
Whirl sign due to tightly twisted mesenteric vessels
“Balloons-on-strings”: Dilated SB tethered by stretched mesenteric vessels
• Strangulating SBO: Impaired blood supply to SB
Absent, decreased, or delayed bowel wall enhancement
Bowel wall thickening (edema or hemorrhage)
Mesenteric and interloop edema ± ascites
Vessels: Congested, thrombosed, or obscured
Obscured margins among affected SB segments
TOP DIFFERENTIAL DIAGNOSES
• Adynamic or paralytic ileus
• Aerophagia
• Colonic obstruction
• Cystic fibrosis
CLINICAL ISSUES
• Most common causes: Adhesions (∼ 60%), hernias (15%), tumors (∼ 15%; metastases > primary tumor)
• Up to 80% of adhesive SBOs resolve spontaneously
• Mortality > 25% if symptoms persist and surgery postponed > 36 hours
• Mortality is 100% for untreated strangulated SBOs
DIAGNOSTIC CHECKLIST
• CT diagnosis of closed loop or strangulated (ischemic) SBO is crucial for directing prompt surgical intervention
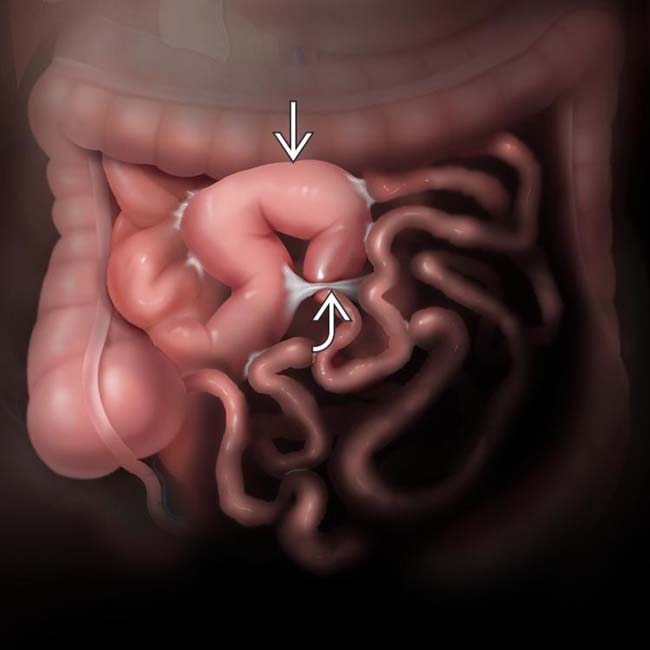
(Left) Anteroposterior graphic depiction of a small bowel obstruction (SBO) due to an adhesive band. Note the dilation of the proximal small bowel , as well as the adhesive band .
(Right) In this patient with abdominal pain, distention, and nausea, a supine film of the abdomen shows no obvious dilation of small bowel (SB).
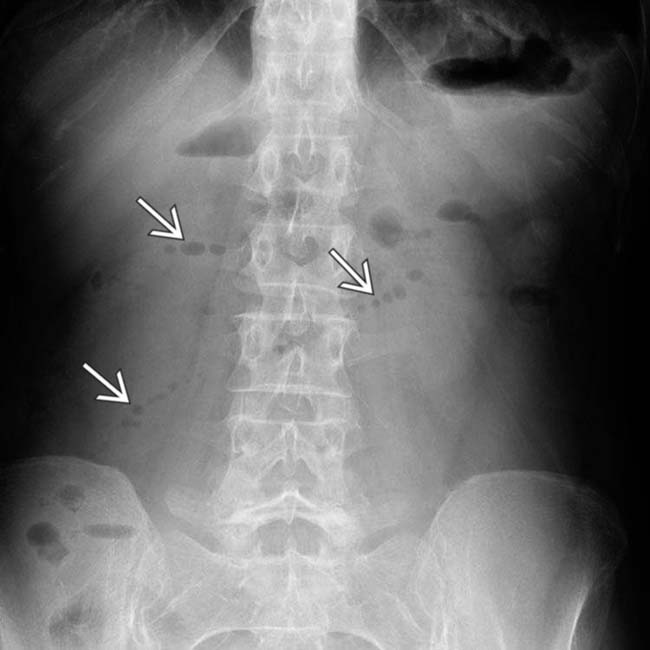
(Left) An upright film in the same patient shows a string-of-pearls sign , indicating gas within fluid-distended, obstructed segments of SB.
(Right) Axial CT section in the same patient shows collapsed distal SB , but massive dilation of proximal SB segments with only small bubbles of intraluminal air , accounting for the string-of-pearls sign. An adhesive SBO was confirmed at surgery.
TERMINOLOGY
Abbreviations
• Small bowel obstruction (SBO)
Definitions
• Obstruction or blockage of ≥ 1 SB segments by intrinsic or extrinsic narrowing of SB lumen
IMAGING
General Features
• Best diagnostic clue
Identification of transition zone between dilated and collapsed bowel is critical to define presence, site, and cause of obstruction (all better determined on CT than on plain films)
• Size
Small bowel loops > 3 cm diameter on radiographs, 2.5 cm on CT (magnification effect on plain films)
Radiographic Findings
• Radiography
Supine abdomen with upright or decubitus views
– Dilated SB loops with air-fluid levels on upright or decubitus radiograph
Can miss SBO (fluid-distended bowel not evident on plain films)
String-of-pearls sign: Small air bubbles within fluid-distended bowel seen on supine view
Fluoroscopic Findings
• Enteroclysis or SB series
Passage of enteric contrast into colon excludes complete SBO
Transition may define location, degree, cause of obstruction
– e.g., angulated segment with distortion of folds suggests adhesive SBO









 , as well as the adhesive band
, as well as the adhesive band  .
.
 , indicating gas within fluid-distended, obstructed segments of SB.
, indicating gas within fluid-distended, obstructed segments of SB.
 , but massive dilation of proximal SB segments
, but massive dilation of proximal SB segments  with only small bubbles of intraluminal air
with only small bubbles of intraluminal air  , accounting for the string-of-pearls sign. An adhesive SBO was confirmed at surgery.
, accounting for the string-of-pearls sign. An adhesive SBO was confirmed at surgery.






 Hernia
Hernia Peritoneal carcinomatosis: Omental and peritoneal masses, dilated bowel loops, multiple transition zones
Peritoneal carcinomatosis: Omental and peritoneal masses, dilated bowel loops, multiple transition zones






 Classic triad: Ectopic calcified stone and gas in gall bladder/biliary tree and SBO = gallstone ileus
Classic triad: Ectopic calcified stone and gas in gall bladder/biliary tree and SBO = gallstone ileus















