George M. Bridgeforth and George Holmes
A 45-year-old woman fell. On physical examination, she has medial and lateral right ankle pain and swelling.

CLINICAL POINTS
- Pain-limited ambulation is characteristic.
- Heel pain (calcaneal fracture) may be present.
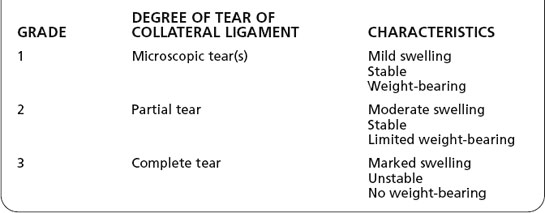
- Tears of collateral ligaments vary in severity.
- There may be an associated talar or fifth metatarsal (Jones vs. styloid) fracture.
Clinical Presentation
Tears of the collateral ligaments of the ankle result in ankle sprains. Such tears are classified on the basis of severity. Clinically, there are three grades of ankle sprains, depending on the degree of the ligament tear (Table 20.1). Ankle ligaments are grouped into two categories—lateral collateral ligaments and medial collateral ligaments. The mechanisms of injury involved in tearing of collateral ligaments are as follows:
- Medial collateral ligament: ankle eversion with impact (valgus force) (Fig. 20.1)
- Lateral collateral ligament: ankle inversion with impact (varus force) (Fig. 20.2)
Patients with torn ankle ligaments complain of pain, swelling and bruising, and tenderness. Loss of functional ability, including weight-bearing, is high. Pain-limited range of motion is characteristic.
The Ottawa rules were developed by a group of Canadian emergency physicians as a set of guidelines that assist physicians in assessing ankle injuries. A concise synopsis of the Ottawa rules for foot and ankle injuries recommends that radiographs should be obtained in the following circumstances:
- There is point tenderness anywhere along the posterior aspect of the distal 6 cm of the medial or lateral malleolus.
- There is an inability to take four steps during an examination.
- There is tenderness over the navicular bone at the base of the fifth metatarsal.
The Ottawa rules have excellent sensitivity. According to many studies, the sensitivity is well more than 90% (perhaps even 100%). However, the specificity varies between 15% and 30%. In other words, if any one of the previously mentioned criteria is met, the physician should obtain radiographs. However, the complete absence of any of the Ottawa findings may not rule out an ankle fracture in selected cases. Until there is malpractice legislation to protect physicians who adhere strictly to the Ottawa rules, the individual physician is advised to use his or her own discretion.
When assessing an acute ankle injury, it is always necessary to check for tenderness of the talus and the fifth metatarsal. If there is tenderness of the talus (especially with dorsiflexion) or the fifth metatarsal, then radiographs of the foot should be ordered as well. Fifth metatarsal fractures are often missed because the examiner looks only at the ankle injury. Also, the talus should be palpated, to check for talar pain with ankle dorsiflexion, which may indicate an associated talar fracture. In addition, the proximal fibula should be checked for pain and tenderness (Maisonneuve fracture or spiral fracture of the fibula that extends to the proximal fibula). This is associated with a torn distal tibiofibular syndesmotic complex. Heel pain (calcaneal fracture) is also a possibility.
Table 20.1 Acute Ankle Sprains
The examiner should use the anterior–posterior drawer test to check for ankle instability (torn anterior tibiofibular ligament). The examiner stabilizes the ankle with one hand and cups the heel with the opposite hand, checking for forward movement of the subtalar joint. A positive test indicates a torn anterior tibiofibular ligament.
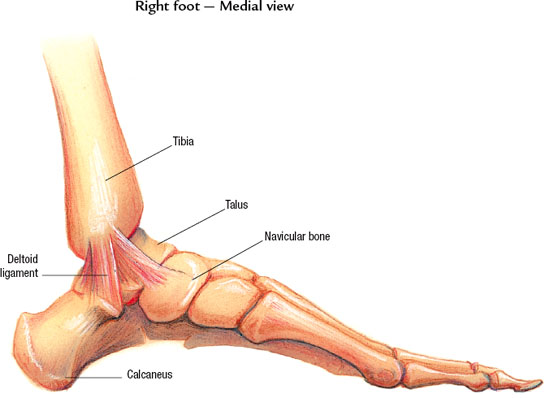
FIGURE 20.1 The medial collateral ligament is formed by the broad-shaped deltoid ligament. It helps prevent subluxations of the ankle during eversion. (Courtesy of the Anatomical Chart Co.)
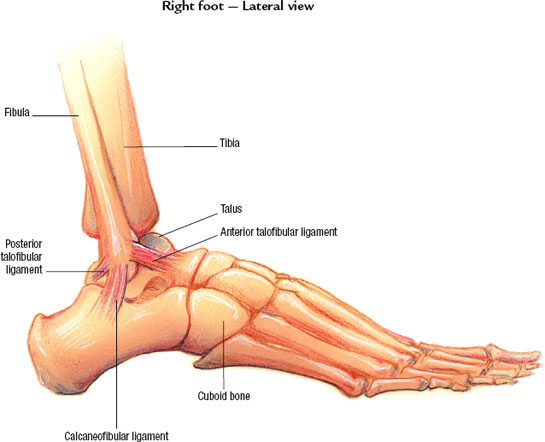
FIGURE 20.2 Lateral collateral ligaments of the ankle: the anterior talofibular ligament, the posterior talofibular ligament, and the calcaneofibular ligament. They prevent subluxation of the ankle during inversion. (Courtesy of the Anatomical Chart Co.)
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


