Transient Hepatic Attenuation or Intensity Difference (THADs and THIDs)
Become isodense (isointense) on venous and delayed phases
• Pseudolesions on nuclear medicine studies
e.g., “hot” accumulation of Tc-sulfur colloid in left lobe of liver in patients with SVC obstruction
“Hot” accumulation of FDG within THAD on PET/CT
TOP DIFFERENTIAL DIAGNOSES
• Hypervascular liver mass
• Focal confluent fibrosis
• Hemangioma
• Focal sparing with fatty liver
PATHOLOGY
• THAD due to decreased portal flow
Segmental, peripheral portal vein thrombosis
Direct compression or occlusion of portal vein by mass
Elevated sinusoidal pressure (e.g., due to biliary obstruction)
• THAD due to increased arterial inflow
Peripheral AP shunts in cirrhosis
Hypervascular masses may draw ↑ flow (siphon effect)
Post-traumatic or congenital AV fistula
• 3rd inflow alternative or additional source of venous flow to liver (e.g., SVC occlusion)
DIAGNOSTIC CHECKLIST
• Check portal venous phase images for subtle mass at apex of wedge-shaped THAD
(Left) Arterial phase CECT in a man recovering from abdominal gunshot wounds shows hyperenhancement of the anterior right lobe segments of the liver due to septic thrombosis of the anterior branch of the right portal vein .
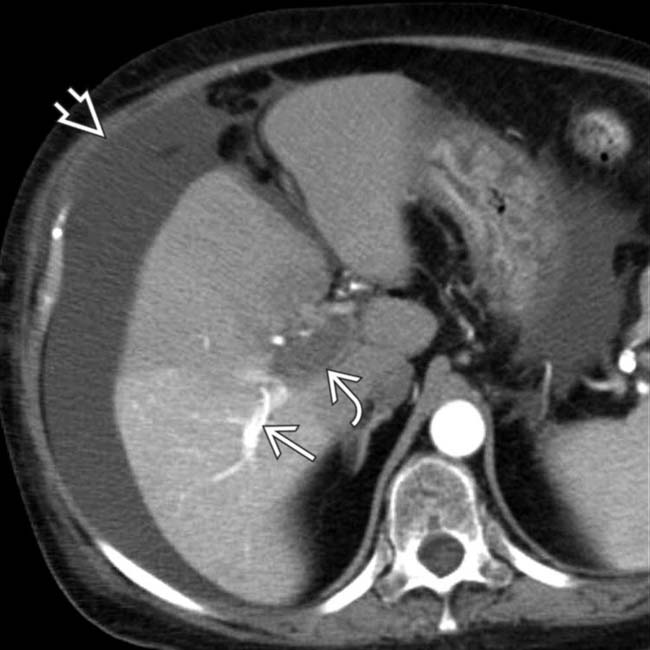
(Right) CECT of an elderly man with septic thrombophlebitis due to diverticulitis shows hyperperfusion of the anterior right lobe of the liver due to thrombosis of the anterior branch of the right portal vein and compensatory increased flow from the hepatic artery .
(Left) Arterial phase CECT of a 54-year-old woman with a hypercoagulable condition shows thrombosis of the posterior branch of the right portal vein . Compensatory increased flow through the hepatic artery accounts for the posterior segmental transient hepatic attenuation difference (THAD). Ascites is also noted due to hepatic injury from the portal vein thrombosis.
(Right) Portal venous phase CECT in the same case shows uniform enhancement of the liver, the portal vein thrombus , and ascites .
TERMINOLOGY
Abbreviations
• Transient hepatic attenuation difference (THAD)
• Transient hepatic intensity difference (THID)
Definitions
• Transient increase in hepatic attenuation (or intensity) during arterial phase CT (or MR) due to regional variations in balance between hepatic arterial and portal venous blood flow
IMAGING
General Features
• Best diagnostic clue
Wedge-shaped areas of increased attenuation on arterial phase imaging
– Become isodense (isointense) on portal venous and delayed phases
• Location
Peripheral, extending to capsular surface of liver
• Size
Variable, depending on etiology
– Often segmental or lobar, especially with neoplastic etiology
• Morphology
Straight margins, wedge-shaped
– Usually subsegmental
Segmental or lobar THADs should have identifiable etiology
Small subcapsular THADs more commonly occur in setting of cirrhosis with no focal lesion identified
Rounded lesion at apex of wedge (or triangle) usually represents neoplastic etiology for THAD
Imaging Recommendations
• Best imaging tool
CECT with arterial and portal venous phase imaging
• Protocol advice
Obtain arterial phase 25-40 seconds after IV contrast bolus
– Must have adequate volume (> 100 mL) and rate (≥ 3 mL/sec) of IV contrast administration
Portal venous phase 60-80 seconds after IV bolus
CT Findings
• Area with straight margins and wedge-shaped morphology peripherally in liver on arterial phase imaging
Becomes isodense and inconspicuous on venous and delayed phase images
• May demonstrate focal hepatic or perihepatic mass, or portal or hepatic vein thrombosis as specific cause of THAD
MR Findings
• Arterial phase of gadolinium-enhanced MR shows areas of hyperenhancement (THID)
Becomes isointense to liver on venous and delayed phases
Ultrasonographic Findings
• No corollary findings, except with contrast-enhanced US
e.g., with microbubble contrast agent
Nuclear Medicine Findings
• Same foci and pathophysiology of THAD may result in pseudolesions on nuclear medicine studies
e.g., “hot” accumulation of Tc sulfur colloid in left lobe of liver in patients with SVC obstruction
“Hot” accumulation of FDG within a THAD on PET-CT
– Easily misinterpreted as a focus of tumor
DIFFERENTIAL DIAGNOSIS
Hypervascular Liver Mass
• Hepatocellular carcinoma, focal nodular hyperplasia, or hypervascular metastases (carcinoid, neuroendocrine most common)
• Usually spherical or oval, not wedge-shaped
• May show washout on portal venous phase imaging
• May be associated with arterioportal shunting or THAD
But mass should be identified as separate from THAD
Mass is typically spherical lesion
May cause rounded lesion at apex of wedge-shaped THAD
Focal Confluent Fibrosis
• Capsular retraction and volume loss in cirrhotic liver
Only gold members can continue reading. Log In or Register to continue
 e.g., “hot” accumulation of Tc-sulfur colloid in left lobe of liver in patients with SVC obstruction
e.g., “hot” accumulation of Tc-sulfur colloid in left lobe of liver in patients with SVC obstruction






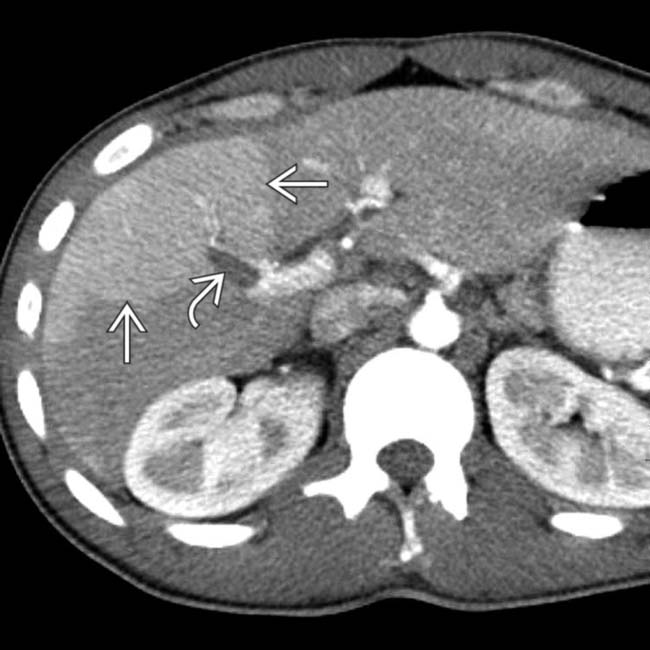
 due to septic thrombosis of the anterior branch of the right portal vein
due to septic thrombosis of the anterior branch of the right portal vein  .
.
 due to thrombosis of the anterior branch of the right portal vein and compensatory increased flow from the hepatic artery
due to thrombosis of the anterior branch of the right portal vein and compensatory increased flow from the hepatic artery  .
.
 . Compensatory increased flow through the hepatic artery
. Compensatory increased flow through the hepatic artery  accounts for the posterior segmental transient hepatic attenuation difference (THAD). Ascites is also noted
accounts for the posterior segmental transient hepatic attenuation difference (THAD). Ascites is also noted  due to hepatic injury from the portal vein thrombosis.
due to hepatic injury from the portal vein thrombosis.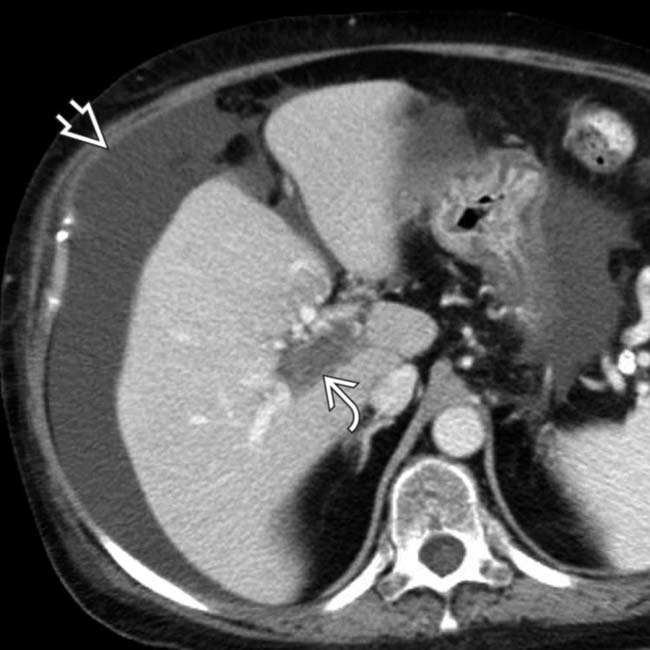
 , and ascites
, and ascites  .
.






















